From Clinic To Practice 6: Chronic “Hip Flexor Strains” in Gymnasts

One of the areas I have spent the most time researching, treating, and brainstorming on is hip pain in gymnastics. When first starting to treat many gymnasts, I couldn’t quite seem to wrap my head around why so many athletes suffered from chronic, debilitating “hip flexor strains” and groin pain that caused them to lose months of training. By studying some great new research (find more here, here, here, here, and here), talking with orthopedic surgeons who specialize in hip instability, and developing ideas with the gymnasts I coach/treat, I have progressed my thinking on this challenging issue quite a bit.
To help the gymnastics coaching and medical community, I want to share a new “From Clinic To Practice” post that highlights these concepts in two cases of hip pain in gymnasts.
Also keep in mind, I recently wrote a comprehensive review of Gymnastics injuries and rehabilitation, which is all now available for free download here,
Table of Contents
The Gymnastics Medical Injuries Guide
- Understand the most common injuries in male and female gymnastics, why they occur, and how to prevent them
- Read about the most current science on injuries and rehabilitation in gymnastics
- Get tips on the latest injury risk reduction and rehabilitation practices
We take our privacy seriously and will never share your information. Click here to read our full privacy policy.
This Part 1 will help coaches, gymnasts, parents, and medical providers get a sense of where the research is moving for why these hip problems tart in the first place.
Background To Their Hip Injuries
The first athlete was actually an optional gymnast on our team who had her injury start at the end of last competitive season. Just like any other gym we face injuries within our team and address them appropriately. Although it was very unfortunate timing on the end of her competitive year, it gave me first hand experience for managing it and helping her back over the summer. The other was an optional gymnast who came to Champion for treatment after 2 years of struggling and being on the verge of quitting (thanks to them for permission to use photos below).
These two gymnasts, along with many others I have worked with, have a surprising overlap in patterns for their injury development. They all
- Had sudden onset of hip pain in the front/groin area that hurt to touch and caused notable limping
- Had pain that was made worse by extending their hip or rotating out, splits, leaps, running, kipping, beam series, and pulling into flip shapes.
- Struggle to return to gymnastics fully due to flexibility, skill, and volume they are training at
After needed rest, rehabilitation, figuring out the pattern of injury, and training modifications, I’m happy to say that as of now both are back to training pain free. Next, let me explains some of my current thoughts on these types of injuries.
Understanding Why Their Hip Injuries Occurred
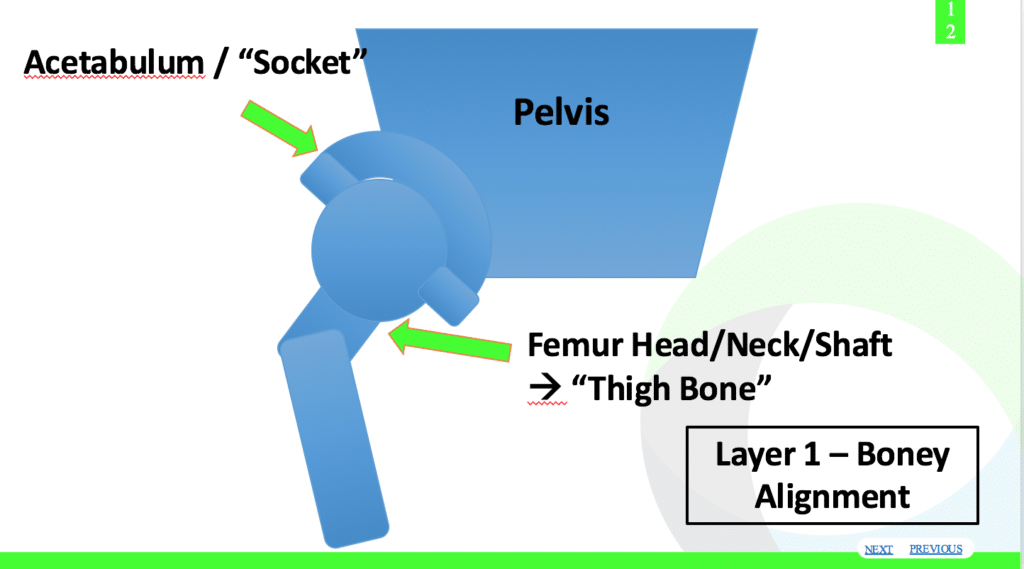
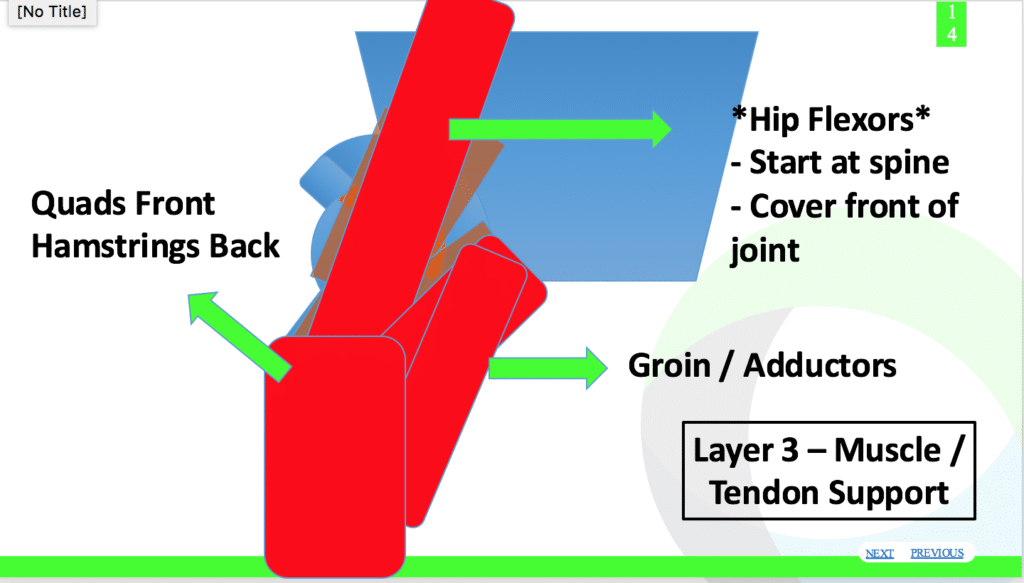
We have to understand the anatomy and remember there is much more to the hip than just hip flexors and groin muscles. As Draovitch and Kelly outlined in this article, the hip can be though about as having “layers”.
Layer 1 being the bones and their alignment, Layer 2 being the more passive stabilizers like the ligaments/joint capsule/labrum, and then Layers 3 and 4 being the dynamic muscular stabilizers. Together these layers help keep the hip joint in place, while also creating movement and absorbing force.
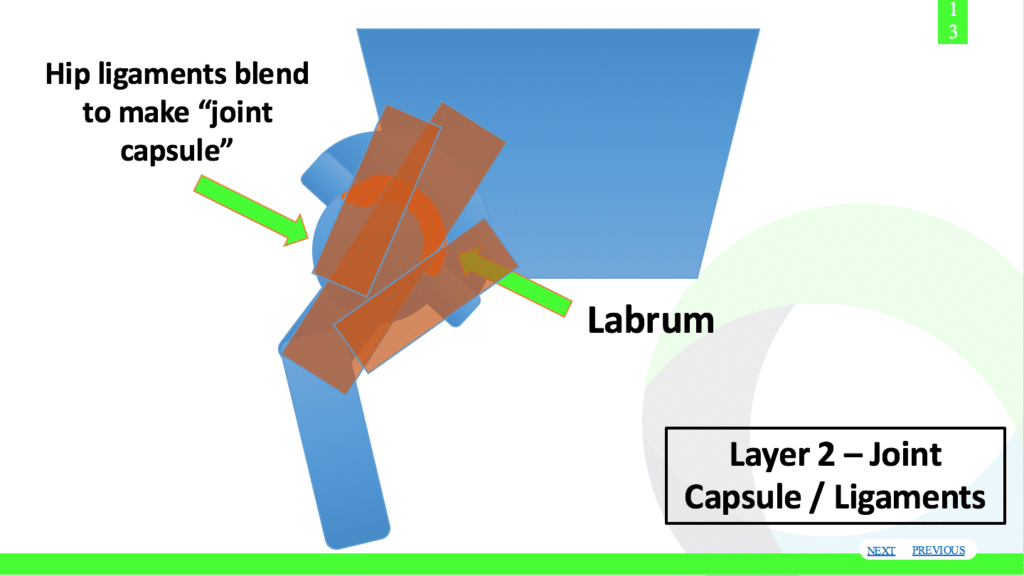
Remember that hip injuries are a beast of a topic, with hundreds of possible overlapping factors behind it. As I wrote about in this article, I think these hip flexor pains may actually (not always) be much more serious issues such as the deeper hip layers of the ligament, capsule, and labrum micro damage occurring over time. It may feel like it is on the surface as muscular strain, or that muscle could be irritated as a secondary reason, but deep problems likely exist.
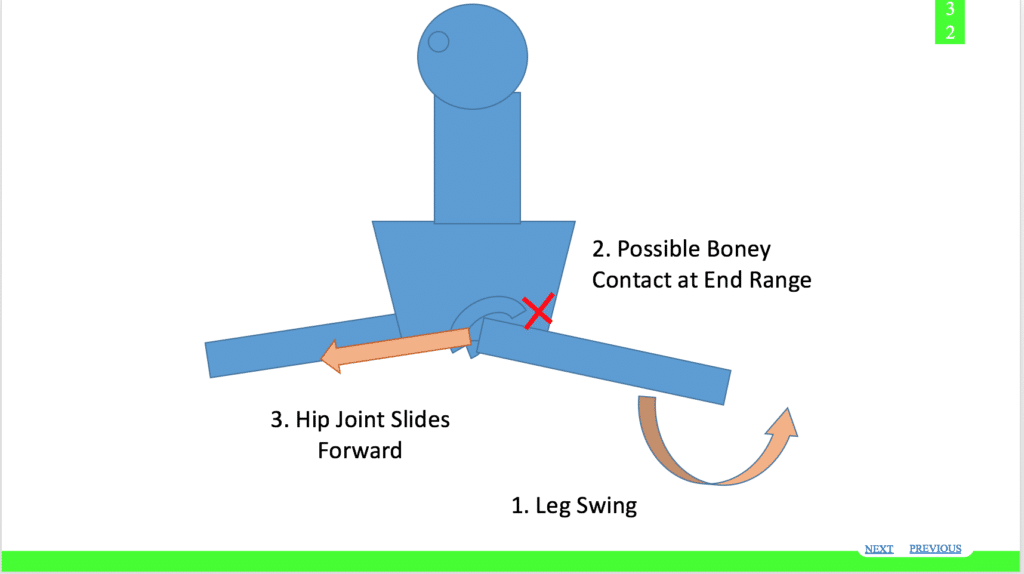
The end range of hip motions backwards and out (think back leg of split leap) tends to be where a lot of these issues occur. As this recent great study outlines, this end range of motion can potentially put lots of stress on the front of hip joint and ligaments.
I personally feel that dynamic end range motion without appropriate strength/control, may be sparking lots of irritation in gymnasts hips over time. The same concept can apply to straddling and front kicking. This combined with increasingly difficult gymnastics skills, non individualized and possibly out dated flexibility programs, and underdeveloped hip strength quickly snowball into serious issues.
This ligament, capsule, and sometimes labrum area are even more taxed when reaching end range of motion due to the leg bone possibly bumping into the back of hip socket. I outlined this in the picture above, but with both end range straddle, backward, and frontward kicking the two bones may essentially fulcrum on each other to cause more stress. It may create a pinch type feeling on one side, with a painful stretch or pull sensation on the other. This is why I feel the hip flexors or groins gets overstretched from behind and reflexively tighter to protect the joint when this sliding may occur, falsely leading to “hip flexor strains” or “groin strains” as a diagnosis. Overtime the joint, ligament, and labrum can become injuries leading to some serious issues.
It is challenging to train these large ranges for gymnastics skills, but I think it can be done if you take time to think about the concepts. Here are a few of the more common themes I find in many gymnasts with hip pain. I by no means feel they are absolute, but are patterns I think are important for these types of cases.
1. Naturally Lax Gymnasts Lacking End Range Strength
Both of these gymnasts, as well as many other gymnasts I have treated for hip pain tend were naturally hyper mobile. People argue that sometimes these gymnasts appear “stiff” not having full splits and bridges but soft tissue flexibility problems are different than underlying ligament laxity. It is very possible, and I find quite common, for gymnasts to acquire limited soft tissue flexibility from training while still having notable joint hyper mobility that causes shoulder and hip issues. I personally believe training over time, along with some protective guarding create loses of hip mobility over time in gymnasts.
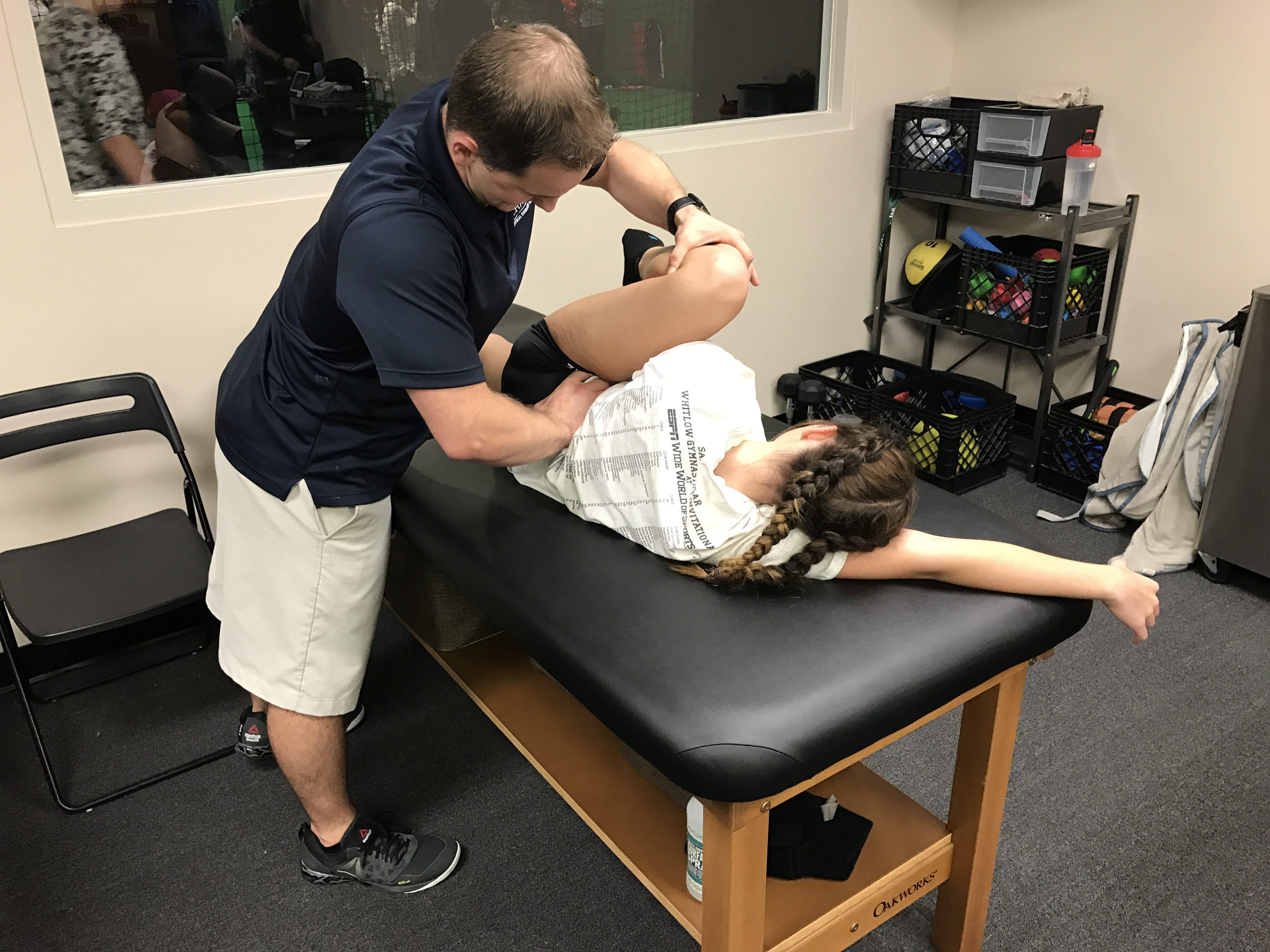
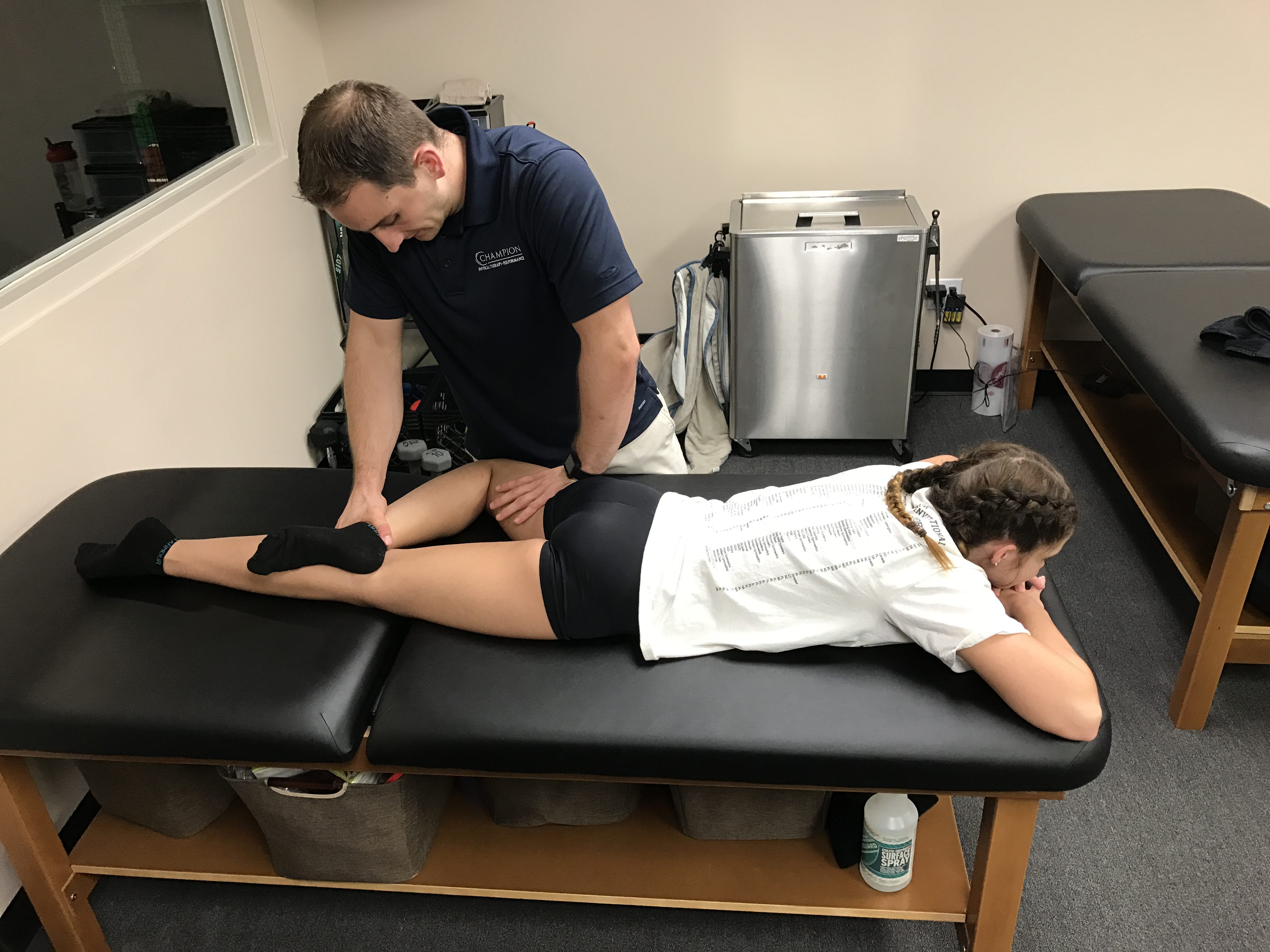
Paired with this concept is that many gymnasts I see who have hip pain tend to be very strong/controlled in their mid range of motion, but not at their end ranges of motion. We have to make sure the strength and active mobility drills we train replicate the full range of motion. This allows the active muscular stabilizers to theoretically take pressure off the more passive static ligament/capsule/labrum stabilizers. Take for example this young gymnast, who was experiencing hip pain during needle kicks due to her lack of end range control and strength.

2. Medical / Assessment Tests That Weren’t Gymnastics Specific Enough
This part of the story is definitely from the other side of the fence in the medical community. In the cases where gymnast came to see me at Champion, almost all of them had a common overlap that the medical providers assessing them did not fully understand gymnastics or apply specific enough tests to detect provocative issues.
I’m definitely not pointing fingers at anyone, as a few years ago I was in the same position scratching my head. That being said, we must make sure we are accurately assessing and diagnosing these micro instability based injuries. I have combined some surgical research with case reports and my own thoughts to come up with a hand full of tests I use to try and replicate skills that are provocative (split leaps, end range back leg splits, sprinting, end range straddles). These are for the medical providers out there.

Apprehension/Shearing in Split Pelvis Position
End Range Abduction Fulcrum Impingement
Prone Figure 4 Anterior Shearing

Prone End Range Extension/ER Shearing
Also, another issue I see popping up is that the rehabilitation is not nearly challenging enough to build hypertrophy, power development, and high level dynamic stability at end ranges. I will cover this more next week in Part 2.
All For Part 1
In the sake of not going too long with this post, I’m going to stop here.I feel fortunate newer information is surfacing that I can use with my background to help better treat athletes with these issues.
Next week I will discuss some other concepts of these types of cases that relate to why I feel these injuries occur, and then discuss some rehabilitation concepts. Thanks for reading, and best of luck!
– Dave Tilley DPT, SCS
References
- DumountGD. Hip Instability: Current Concepts and Treatment. Clinics in Sports Medicine July 2016Volume 35, Issue 3, Pages 435–447
- Skendzel, et al. The Approach to the Evaluation and Surgical Treatment of Mechanical Hip Pain in the Young Patient.
- Weber, et al. The Hyperflexible Hip Managing Hip Pain in the Dancer and Gymnast. Sports Health: A Multidisciplinary Approach April 23, 2014
- Shibata, K.R., Matsuda, S. & Safran, M.R. Is there a distinct pattern to the acetabular labrum and articular cartilage damage in the non-dysplastic hip with instability? Knee Surg Sports Traumatol Arthrosc (2016).doi:10.1007/s00167-016-4342-4
- Kalisvaart MM, Safran MR. Microinstability of the hip—it does exist: etiology, diagnosis and treatment. J Hip Preserv Surg (2015) 2 (2):123-135.doi: 10.1093/jhps/hnv017






