The Ultimate Gymnastics Flexibility Guide

*Readers Note – This gymnastics flexibility guide is a very long and in-depth blog post. The first few sections of this blog are background and explanation for flexibility methods using scientific research. There is a lot of medical and science nerdiness in there. If you are not into that and are just looking for a particular area of the body without the geeky stuff, please click the table of contents below to jump to a certain section.
Table of Contents
Key Points
- Gymnastics requires significant amounts of flexibility and mobility, which makes it a primary area of training
- It can be very confusing and easily overwhelming, especially with the rapid increase in scientific advances and the internet
- Anyone working with gymnasts should have an understanding of basic anatomy and physiology before assigning flexibility drills
- Although research is conflicting, there appear to be both neurological and mechanical reasons as to why regular flexibility training increases range of motion
- It’s crucial that proper methods are used to reduce joint stress and bias the stretching of soft tissue structures, especially in hypermobile athletes
- Static stretching has a role to play in gymnastics but must be used correctly and at the right dosage. Other forms of stretching like PNF, dynamic stretching, and others appear to be effective when regularly done
- “Consistency over intensity” is a key concept everyone in gymnastics must follow
- Although research is conflicting, self soft tissue care as is seen with foam rolling and other tools may have a role in reducing perceived soreness and increasing blood flow to muscles.
- There are many other important tools such as proper strength training, eccentrics, managing workloads, and regular mobility work that must be considered and used as well, as they are supported by research
- Movement assessments are essential to seeing progress with flexibility
- Screening, soft tissue care, stretching, strength work, eccentrics, and gymnastics specific drills should all be used in flexibility programs
Introduction
There are a handful of topics that are regularly at the center of conversation within the sport of gymnastics. Drill progressions for skills, strength and conditioning, managing fears, and dealing with pain or injury are among the most discussed.
However, in my twenty-five years of being a gymnast, a gymnastics coach, and a Sports Physical Therapist who treats hundreds of gymnasts per year, flexibility is by far what I get the most questions about. It’s for good reason too. Gymnastics requires a significant amount of flexibility for skills to be done correctly and safely. It is also one of the main scoring components that judges evaluate during competitions. If not regularly and appropriately trained, flexibility can become something that really holds an athlete back from making progress in skills or possibly contributes to elevated injury risk.
Between coaching, treating, and consulting in gymnastics around the world, offering advice on flexibility has become a staple in my work. The problem is, between the massive amount of information on the internet, the rapid progression of scientific literature, and the wide range of possible reasons behind why someone struggles with flexibility, it can be absolutely exhausting to learn about and use practically to actually see long term results in the gy.
I meet many well-intentioned gymnastics coaches and parents who are simply looking for an easy to use, but scientifically-backed flexibility program to help the gymnasts they know to increase their flexibility, reduce the risk of injury, and increase their performance.
Many of them tell me that they try searching online, going to clinics or camps, and asking around at gyms about how to help, only to become significantly overwhelmed. They try videos from the internet, are disciplined about stretching at practice and at home, do active flexibility, try different medical providers, and all sorts of home remedies, only to come up short. They tell me they often times find temporary progress, but nothing seems to stick long term and actually show up in their skills. By the end of a few months, they usually just throw their hands up and say “he/she is just unflexible, they have bad genetics”.
Unfortunately, this leaves the gymnast feeling very defeated as if something is wrong with them, not to mention still struggling with skills and possibly at an elevated injury risk. Hip and shoulder flexibility limitations are one main contributor I see clinically to wrist, elbow, shoulder, lower back, and hip injuries in gymnasts.
Why Do So Many Gymnasts Struggle Even When They Stretch Daily?
While genetics and luck do play a little bit of a role when it comes to flexibility, as a whole I tend to disagree that these are the main reasons thousands of gymnasts struggle with flexibility, particularly at the hip and shoulder joint.
It’s my opinion that the sport of gymnastics has yet to use a systematic, individualized, science-based system to flexibility methods in training.
And I’m not off the hook here. As a younger coach and medical provider, I absolutely did not study enough and use proper flexibility methods. After seeing so many gymnasts I worked with struggle, and to be honest suffer overuse injuries, I knew something had to change. I dove headfirst into the scientific literature over 2 years and starting playing around with many new methods in the gym and clinic.
Flash forward 7 years from that point, with much more education to use and well over 1000 gymnasts treated for medical issues. I now look back to how I coached and trained as a gymnast 10 years ago, and am blown away with all the things I was doing that were not backed by scientific support.
Like many people, I largely got my flexibility methods from lessons that my coaches passed down to me, the advice of other coaches at camps or clinics, and whatever I found on the internet through discussion forums. While some of it was helpful, I found that the majority of it was based on anecdotal evidence, and did not have a really solid grounding in the science of anatomy, physiology, medicine, or strength and conditioning.
I’ve been fortunate that now after learning from many people and textbooks, I really have a good handle on the concepts that seem to work, and those that don’t really tend to make a big difference in the long term. In an effort to help people out, I have decided to for the first time take everything that I possibly know about gymnastics flexibility and put it into one mega-blog post here.
Jargon Note – The medical world typically refers to ‘Flexibility‘ as the maximum range of motion a joint can passively reach, including the length of all structures from the joint level to the soft tissue and neural level. “Mobility‘ tends to refer to the amount of motion someone can actively show on their own. This wraps in not only the passive range but also strength, active control, technique, and many other factors. (18, 38-40) I do think it’s an important distinction, but due to cultural norms for gymnastics, I will not be super specific to go by medical jargon like these terms and more.
Free Flexibility Resources for Download
This guide will have a lot of research and science references in it, but in an effort to keep it not as hard to read, I will footnote those studies using parenthesis and include a large references section below.
We will start with some background anatomy, term clarification, and discuss some of the theoretical reasons certain flexibility methods seem to work. From there I will take a deep dive into some cultural issues that exist in gymnastics, and then conclude with step by step flexibility examples for each main region of the body that gymnasts struggle with including the shoulders, hips, ankles, and wrists. I will then end with some important notes on other joints like the knees, elbows, and spine. I hope that this guide can be a place for everyone in gymnastics to find some useful information without feeling so frustrated and overwhelmed.
Before kicking this off, please keep in mind that I wrote an entire book chapter on gymnastics flexibility, which you can download and find for free here. It goes into much more depth than I will in this blog post. The anatomy and theory, as well as some of the joint based material for this blog are taken from that chapter.
I also have taken some of the most effective and popular flexibility circuits I’ve made for male and female gymnasts and put them into a quick PDF to use in the gym. I call them “10 Minute Gymnastics Flexibility Circuits”
Lastly, I have made a Gymnastics Pre-Hab Guide that includes daily soft tissue work, stretching, and weekly circuits to help with reducing the risk of injuries in gymnasts. It provides full guides for male and female gymnasts to use.
You can download all three here below, and I will also be sure to share lots of other free resources throughout this blog post for people to use at home.
The Gymnastics
Flexibility Guide
- Cutting edge soft tissue, strength, and active flexibility techniques for splits, handstands, and shapes
- Practical traditional stretching methods combined with latest scientific research
- Techniques for increasing flexibility, and making changes transfer to gymnastics skills
We take our privacy seriously and will never share your information. Click here to read our full privacy policy.
Download My New Free
10 Minute Gymnastics Flexibility Circuits

- 4 full hip and shoulder circuits in PDF
- Front splits, straddle splits, handstands and pommel horse/parallel bar flexibility
- Downloadable checklists to use at practice
- Exercise videos for every drill included
Download SHIFT's Free Gymnastics Pre-Hab Guide


Daily soft tissue and activation exercises
Specific 2x/week Circuits for Male and Female Gymnasts
Descriptions, Exercise Videos, and Downloadable Checklists

Background Anatomy and Understanding Hypermobility
I usually start any discussion that I have with coaches or gymnasts related to flexibility on some basic anatomy. It’s important to recognize that the range of motion a gymnast’s hip, shoulder, or other joints display are directly related to their underlying anatomy. Many structures in the body can influence how much each joint moves. In general, these structures can be lumped into the categories of “passive” or “active”, with research outlining this more specifically for the shoulder (1-5) and the hip (5-12)
The passive structures include things like the bones, ligaments, joint capsules, and the inherent boney alignment we are born with. For the most part, these structures cannot change too much unless surgery of some nature is performed, or through adaptation across many years as is seen when children grow or participate in overhead throwing sports from a young age.
The active structures are more what people know about from gymnastics flexibility methods: muscles, tendons that attach muscles to bones, and the nervous system. These structures and systems tend to have much more potential to change through training. As a result, they have more ability to positively increase an athlete’s overall amount of shoulder or hip flexibility.
Beighton’s Testing and Links to Capsular Laxity
Within the sport of gymnastics, a large majority of athletes who get involved have underlying natural hypermobility. This concept simply means the passive structures like the ligaments or joint capsules tend to be already very lax and they naturally may have much less stiffness throughout their body. This is commonly tested with something called a Beighton’s screening. This screen measures hypermobility through looking at elbow hyperextension, knee hyperextension, the ability to touch the floor in a pike stretch, hyperextension of the pinky, and hyperextension of the thumb.
Some studies have correlated a higher Beighton’s score with increased capsular laxity, including this research study linking a Beighton score over 4 to hip capsular laxity (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5400218/) and this study that discusses the links between shoulder capsular laxity and a high Beightons score (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4295707/)
Every young child’s body has certain unique characteristics that may predispose them to success in certain sports. Naturally, hypermobile kids may do well in sports like gymnastics and baseball. Naturally tall kids may do well in sports like basketball or volleyball. Naturally, fast kids may do well in soccer or track and field. The athletes with naturally lax ligaments allow them to get into specific ranges of motion needed for even the most basic gymnastics skills. Handstands, beginner jumps or leaps, and introductory ring or parallel bar skills demand extreme mobility to execute.
This is typically why these gymnasts from a young age enjoy recreational gymnastics. Their hypermobility, along with any underlying talent or great coaching they obtain to control this range of motion, allows them to be quite successful at an early age. They can easily perform flexibility drills, achieve tumbling or bar lines, create basic gymnastics shapes and proceed through lower-level skills. This is not always the case, but the vast majority of young gymnasts fall into this category once you move past the recreational level.
These children are often detected through an early talent identification and are quickly put into competitive team tracks. Coaches notice their flexibility or ability to perform lower-level skills well. These gymnasts typically have natural flexibility but may struggle to build strength and power during training. Coaches understand that with more strength and technique training in a more structured environment they can progress quickly.
There are some cases where young children do not have natural hypermobility but are gifted in their bodyweight strength abilities. They tend to be more biased towards strength or power and less towards inherent flexibility. These cases are much less frequent in gymnastics but do exist. I have worked with many athletes that tend to be stiffer, but because of their incredible natural power, they succeed early on in gymnastics.
This “natural selection” type introduction to gymnastics presents an essential background foundational concept of flexibility training. Due to many gymnasts having inherent hypermobility, we do not want to place excessive stress on the ligaments and joint capsules of athletes.

Even if a young athlete does fall into the category of being not naturally hypermobile but powerful, we still should gravitate away from putting excessive stress on the passive structures like bones, joint capsules, and ligaments. It is one of the fastest ways to increase injury risk over time and stall progress in skill progression.
Without an in-depth medical background to understand human anatomy, the risk to reward ratio of trying to stretch ligaments and joint capsules are incredibly high. There are cases where mobilizing these passive structures is appropriate (after surgery or some other trauma). However, this requires very specialized medical training and must be performed by a healthcare provider who is competent. (13-14)
We all must understand and apply the best available science for hip and shoulder research to avoid excessive strain being placed on the passive structures of gymnasts. Without this knowledge, it is impossible to know whether reported discomfort during stretching is a safe and expected result or an unsafe atypical response.
The reality of flexibility training is there will be some discomfort that is associated with it. This is an expected part of trying to gain flexibility, to a certain degree. However, there is a very fine line between reasonable discomfort and inflicting real pain. There is also a very fine line between stretching the correct active structure to see improvement and overly stressing the incorrect passive structure to cause injury. I generally recommend that not stretch have more intensity than a 3 or 4 out of 10 (0 is no discomfort, 10 is extreme discomfort). Along with this, no stretching shoulder produces excessive soreness longer than the end of the day, as prolonged soreness may indicate microtissue damage.
There are very predictable locations of stretch discomfort that athletes may feel, and other areas that are warning signs of more serious injuries. Stretching the hamstrings typically produces discomfort in the middle of the back of the thigh, not high up in the buttocks where the hamstring attaches to an open growth plate in pre-pubescent gymnasts. Stretching the shoulders overhead typically produces discomfort in the underarms where the lats and teres major are, with some possible chest tissue stretching where the pecs are. They should not produce discomfort on the top of the shoulders, which is more indicative of rotator cuff or soft tissue impingement under the coracoacromial arch. You can read more about hamstring apophysitis here (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6322373/) and shoulder impingement syndromes here (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3945046/)
There has been a large spike in the rate of “hip flexor strains,” “groin strains “, and “cranky shoulders” that I feel is being very much swept under the rug in gymnastics. It directly relates to this conversation on the need to understand anatomy, as well as active and passive structures, and knowing where discomfort is or is not expected.

When an athlete reports hip or shoulder pain, far too many people are jumping to the conclusion and assuming that these reports of pain are just pulled muscles. They say not to worry about it, and that this is something that can be trained through. Although this does happen in gymnastics, there are many times when this is inaccurate and dangerous.
I fear that what many people write off as small strains is actually the start of more serious issues like labral tears, pelvic bone stress fractures, and rotator cuff or biceps tendon damage. Again, without an in-depth knowledge of anatomy, injury mechanisms, and medical imaging, it is tough for someone to tell the difference between a hip flexor strain and a more severe ligament or labral tear. (1, 3, 5, 8-9, 15-16)
In the short term, these smaller flare-ups of pain may not create huge issues. It may very well be a minor strain. Within a few days of modification, advice from a qualified medical provider, and time to heal, issues may resolve quickly. Sometimes in such a high force sport, these bumps and bruises are inevitable.
However, I have seen these types of problems snowball into huge injuries quickly in gymnasts I treat. I have seen what was thought to be a pulled hamstring end up being a pelvic growth plate stress fracture that required six months of time off and rehabilitation. I have seen what was thought to be sore shoulders turn into rotator cuff damage and shoulder instability, requiring surgery to correct. I have also seen what was believed to be a hip flexor strain turn into a large labral tear and career-ending injury.
I do not mean to imply that every report of pain should be panicked over, and that simple muscular strains are not a common occurrence. I more hope to highlight that assuming ongoing pain reports are no big deal and can be trained through, rather than thinking critically about the situation, can be very problematic. With this said, lets review some basic anatomy.
Shoulder Anatomy
The shoulder joint itself can be thought about as a “golf ball sitting on a tee”. The golf ball (ball of the upper arm bone or humerus) is inherently larger than the tee (socket of the shoulder or glenoid fossa). (2, 5)
The bones themselves, and the shape/fit of these bones is often referred to as the first layer of the shoulder joint.

This creates a huge range of mobility for the shoulder joint, but in exchange for inherently less stability. This is unlike the hip joint, which due to having a deeper hip socket (remember hips are built for weight-bearing while shoulders are not) has more inherent stability with less mobility.
Surrounding the ball and socket of the shoulder is something called the “joint capsule” as well as ligaments. The capsule resembles a balloon-type structure that completely surrounds the shoulder joint and serves as a thickened blending of ligaments.(3)
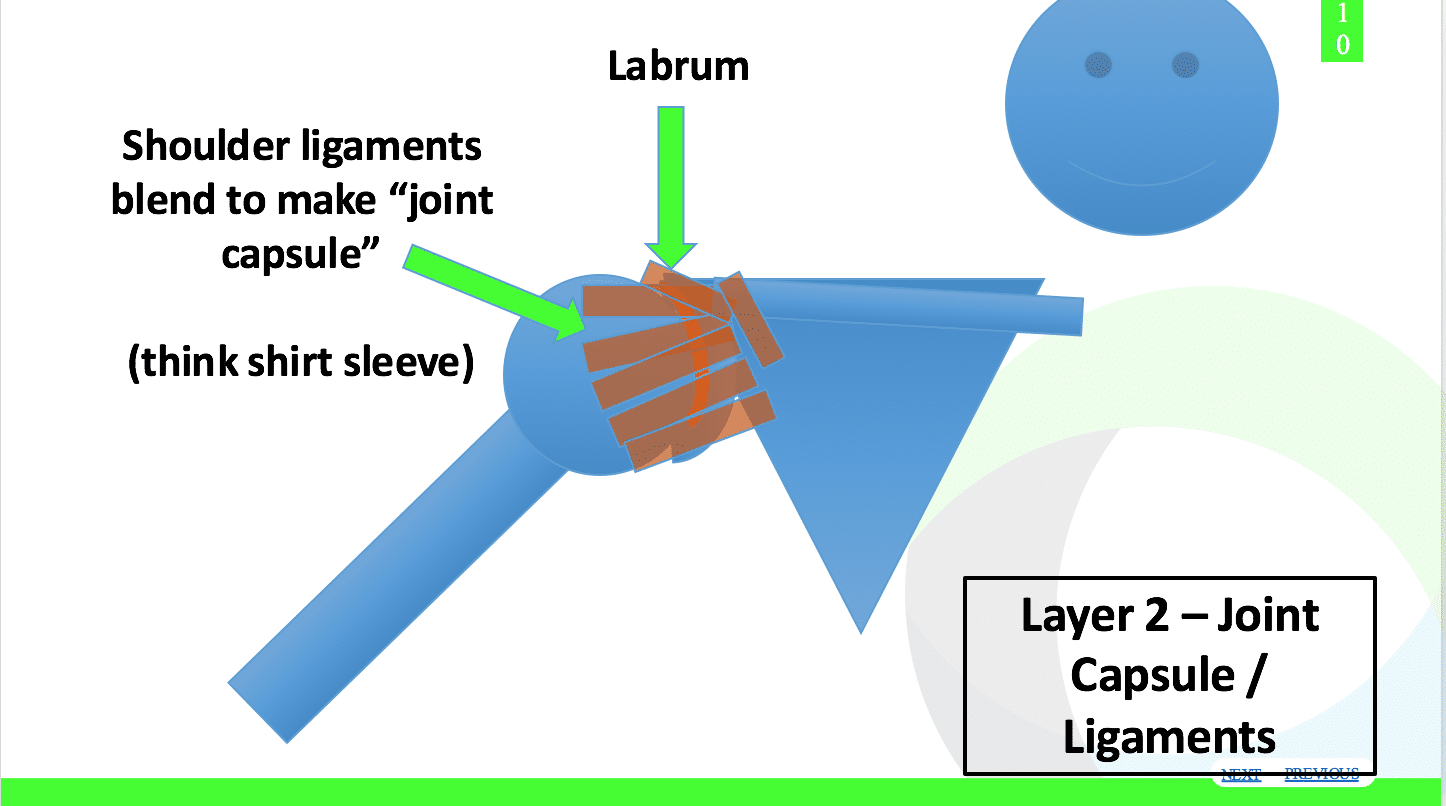
For the geeks like me reading, they more specifically are subdivided into the Superior Glenohumeral Ligament, the Middle Glenohumeral Ligament, the Inferior Glenohumeral Ligament, and the Posterior Glenohumeral Ligament. (3)
The ligaments and joint capsule, along with the alignment of the ball on the socket, create what is known as the “passive” structures or stabilizers. They also represent layer two of the shoulder joint.
To help clarify, many use the analogy of the sleeve of a shirt to visually highlight the joint capsule. If you look down at your arm (and are wearing a shirt) your actual arm within the shirt sleeve represents the first “golf ball on a tee” bony layer, and the shirt sleeve surrounding the arm represents the second layer made up of joint capsules and ligaments.
This second layer of joint capsule and ligaments helps provide more stability to the joint, with different portions of the capsule limiting certain ranges of motion. Just as with the sleeve of a shirt, depending on where your arm is in space, different parts of the shirt sleeve are more taught.
Research in the last decade has been very insightful to learn about certain ligaments and capsule areas that aid in preventing the ball of the shoulder from moving outside the joint and subluxing.
Returning to the analogy of a shirt sleeve, more naturally mobile athletes (gymnasts, baseball players) usually have a “baggier” shirt sleeve. Other more naturally stiff individuals who excel in other sports may have a tighter shirt sleeve. This allows for more or less inherent flexibility, but as always many other factors contribute.
This capsular and ligamentous hypermobility is not inherently a bad thing, as it is part of what makes a gymnast good at the sport. However, as noted in earlier chapters their natural hypermobility can be an area of caution.
We want to make sure we are not over-stretching or overstressing passive structures like the shoulder ligaments and capsules.
For many people in the gymnastics community, it comes down to a professional discussion on taking away overly aggressive flexibility methods, following the science of shoulder anatomy and making subtle changes in training.
In conjunction with this, due to the gymnast’s underlying lack of static stability from the ligaments and capsule, they will need absolutely pristine strength, physical preparation, and dynamic stability from their muscles around the joint. This helps to enhance strength, power, and reduce the risk of instability- based shoulder injuries. This is where the third layer comes into play, the muscular soft tissue.
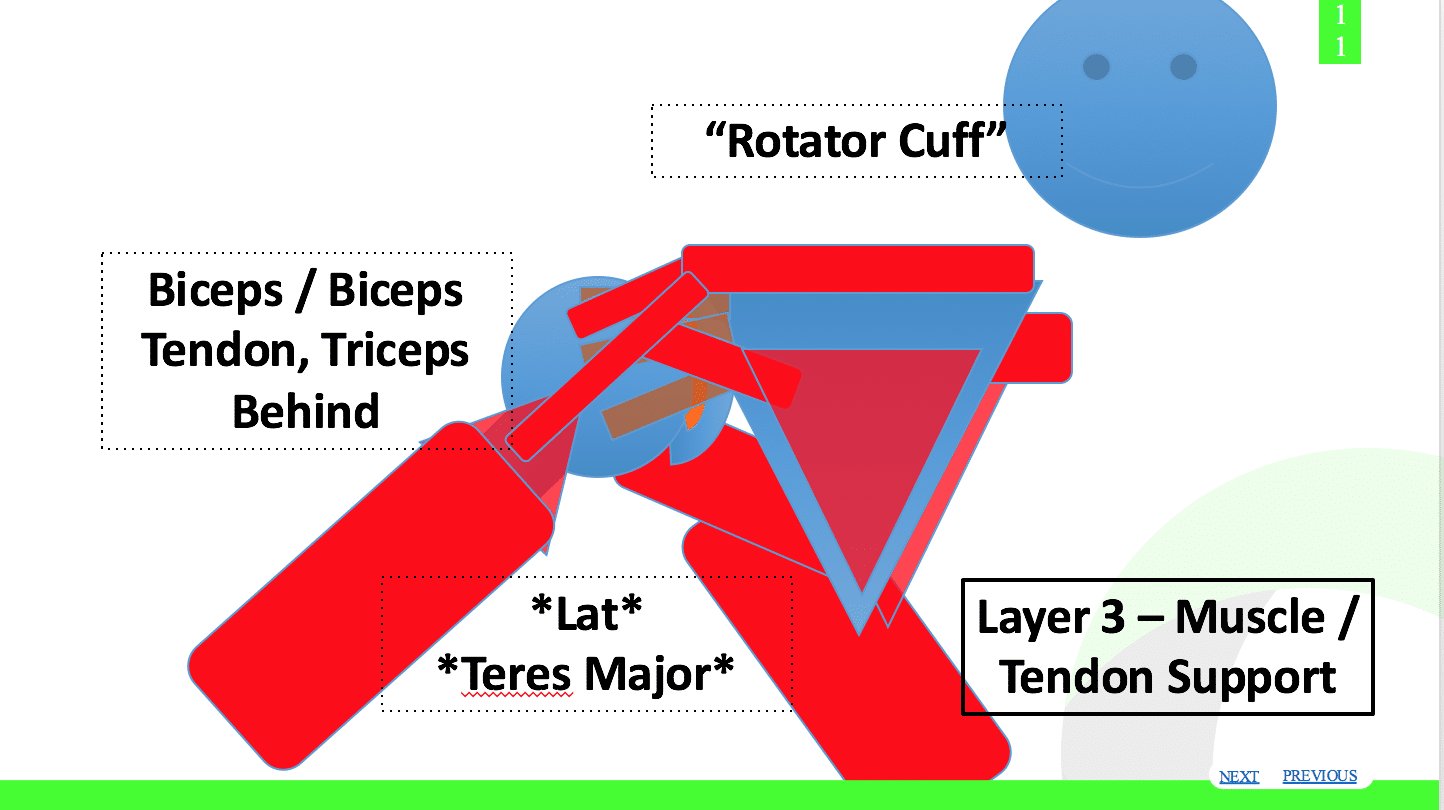
Many people have heard about the muscles of the rotator cuff, biceps, triceps, lats, and so on.
It’s also really important to remember that the upper back, or thoracic spine, and the next play a huge role in shoulder motion. Limitations in thoracic spine flexibility can create a situation where a gymnast is unable to get their arms fully above their head or behind their back. It’s important that gymnasts have their thoracic mobility screened to see if it’s an issue, which I can share more in-depth during the circuit sections.
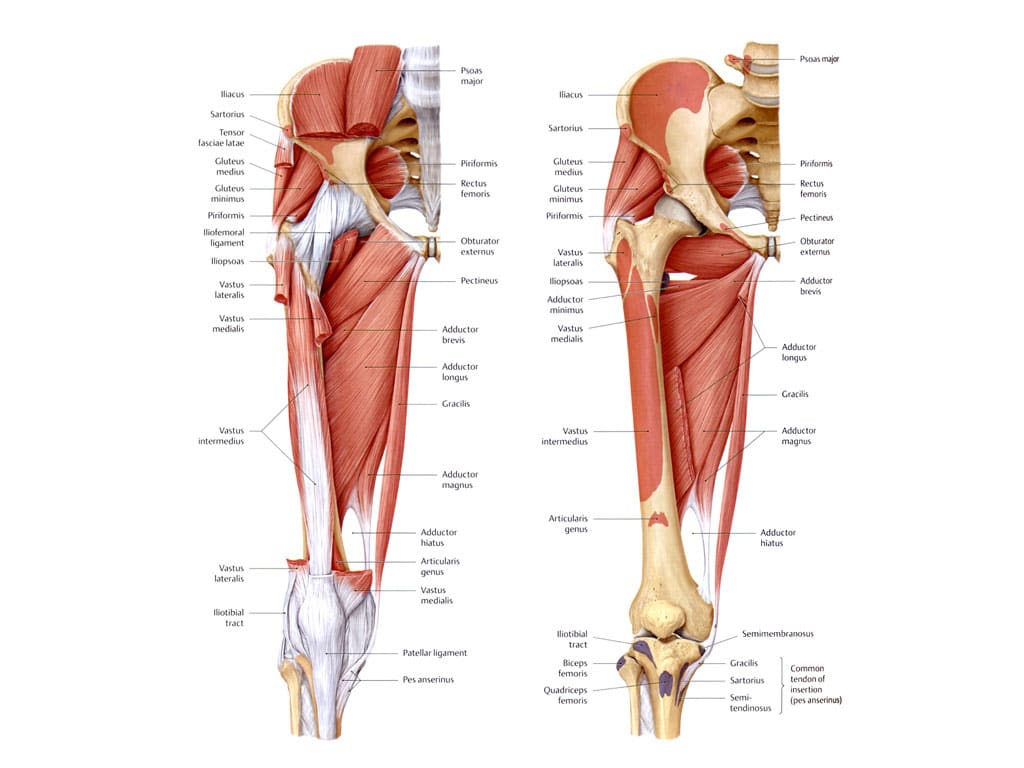
Hip Anatomy
My thoughts on hip mobility and why we choose certain exercises closely echo my thoughts on shoulder mobility, and I again will not go into much depth as this was covered in an earlier chapter.
The research in the world of hip micro instability, labral tears, hip stress fractures, and other injuries commonly seen in gymnasts has been rapidly developing in the last decade. It has been great to see so many great surgeons, healthcare providers, and strength coaches share their thoughts and describe what still needs to be considered. (7-9, 17)
I encourage people to dive into the research of background hip anatomy, as well as the current thoughts on hip injuries within the medical or strength fields. I will offer basic concepts from them in the coming paragraphs as it relates to injuries but can’t stress enough how valuable the articles or textbooks mentioned were to me over the past five years.
As I did with the shoulder section, here are three graphics that walkthrough
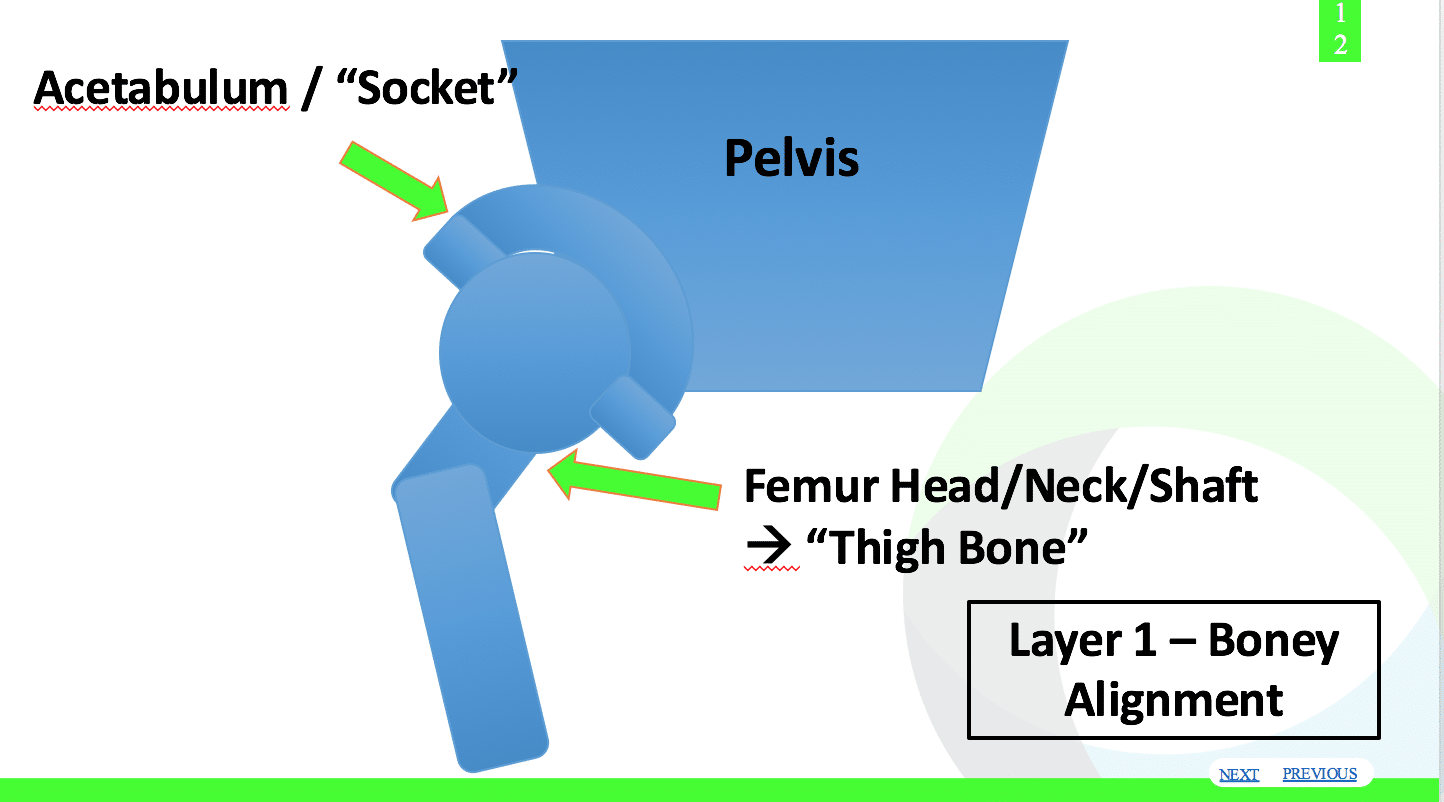
Layer 1 (Bony anatomy)
Layer 2 (Ligaments and capsule) 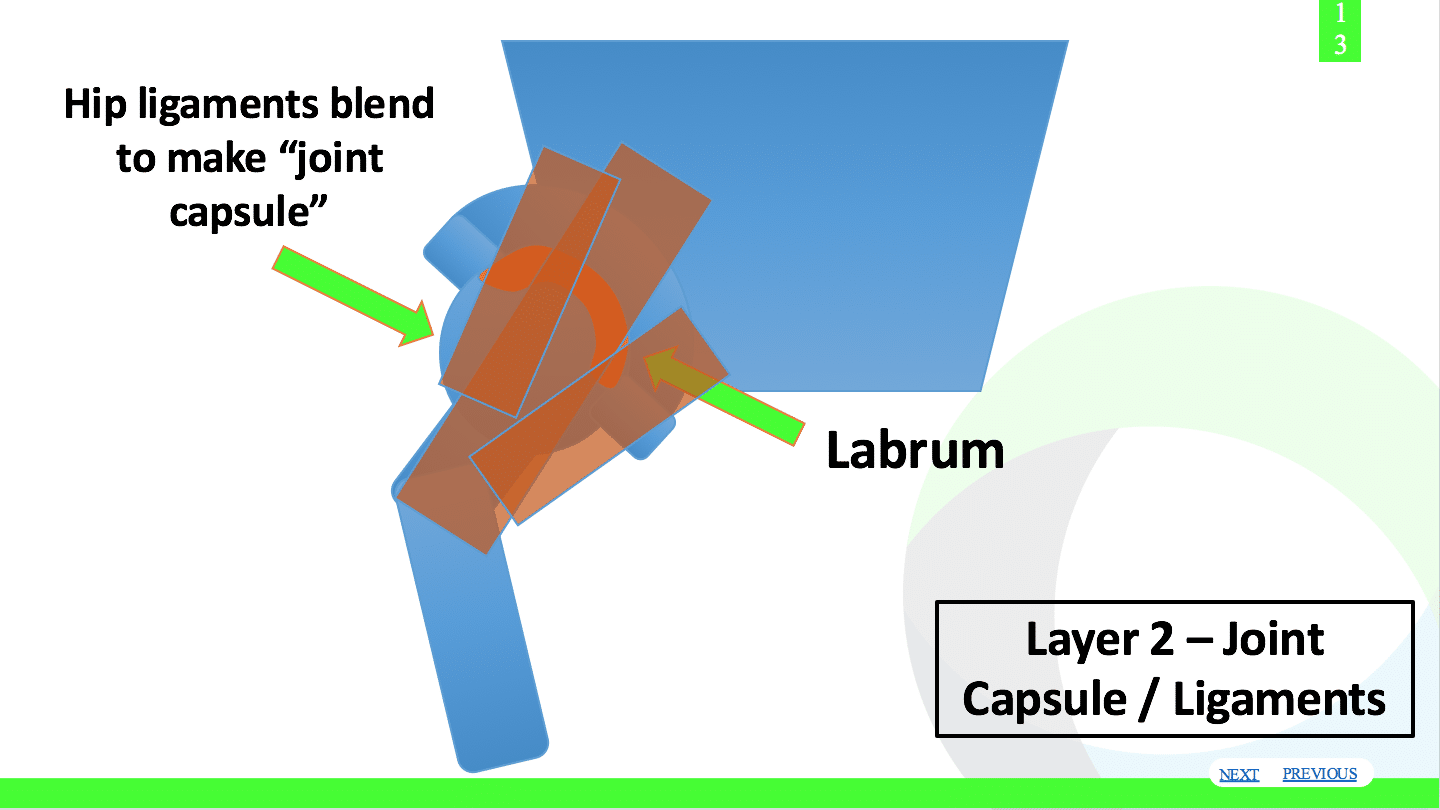
Layer 3 (Muscular examples) 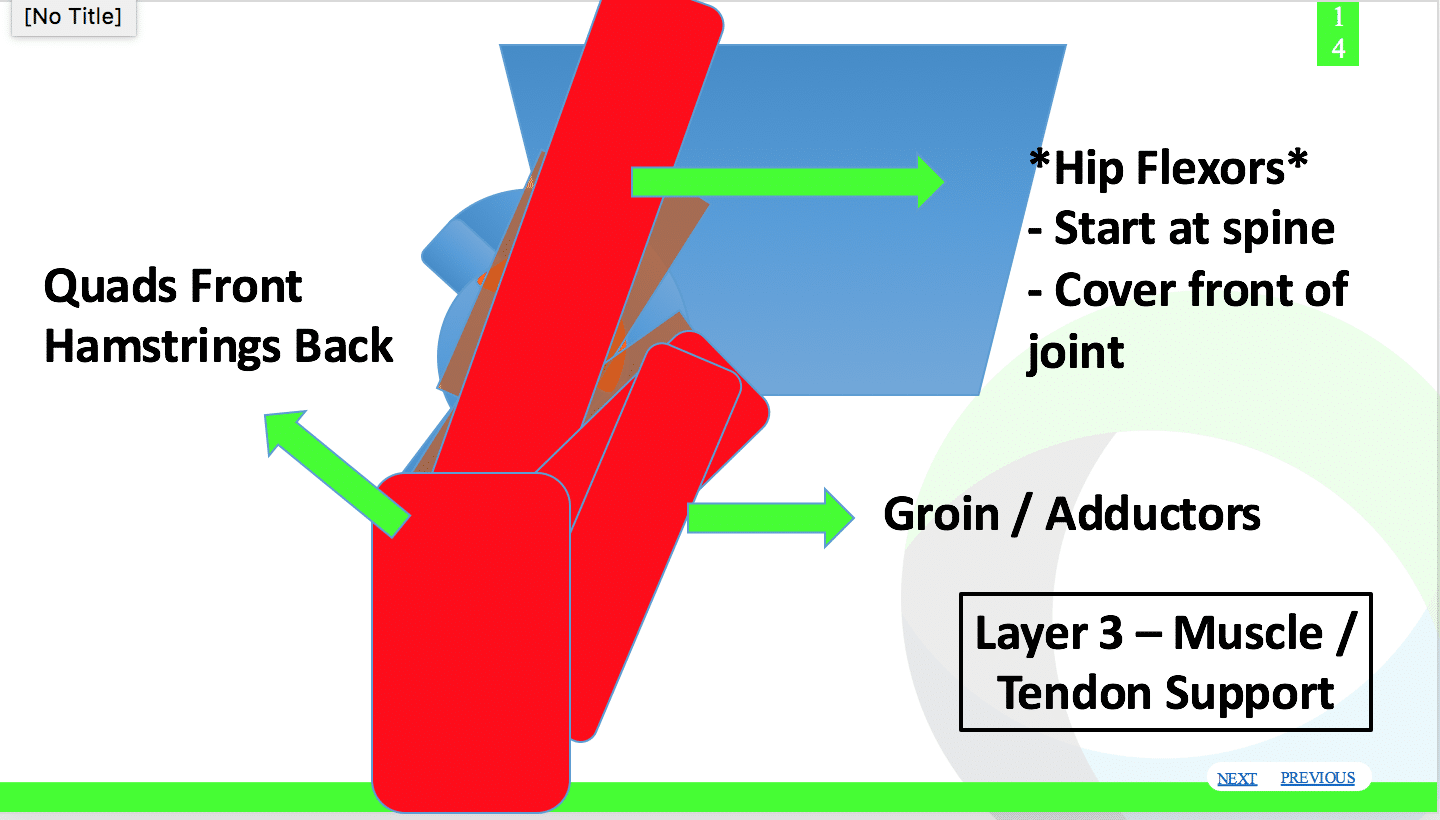
Paralleled to the shoulder, the hip joint is made up of the socket (acetabulum) and the upper thigh bone (femur), with the femoral head serving as the ball.
You may remember the shoulder joint has a very shallow socket, which allows for lots of motion but then creates a situation where stability is needed. The hip is a bit opposite of this, having a deeper socket with more joint congruency. This allows for more inherent weight-bearing stability but may limit the natural mobility the hip can achieve.
Some naturally flexible gymnasts have a bony alignment where the hip socket is not as deep. This creates a situation where the femoral head has more access to move in larger ranges of motion, creating significantly more hip mobility in all planes. These gymnasts typically don’t have to work on flexibility too much to achieve full splits. They also tend to have excessively mobile hip capsules, similar to the shoulder.
The hip socket being overly shallow is referred to as “dysplasia.” Some gymnasts with dysplasia or hypermobile hip capsules never have pain, but some are so far on the continuum of too excessive mobility that it leads to instability and injury.
These gymnasts were born this way. This is usually why they were noticed as a good candidate for competitive gymnastics, as they naturally had full splits and bridges. Like in the shoulder, natural mobility of the hip allows them to move through a greater motion. As mentioned we have to be cautious not to overtax their already hypermobile hip capsules and ligaments during flexibility training.
Reference below – “Microinstabilit of the hip, does it exist?”
With this mobility comes the huge need to be strong, have very good technique, and have exceptional muscular stability. This shallower hip socket, and natural hypermobility, creates a situation where the gymnast cannot afford to have limited dynamic structures for protection.
This is where the third layer of dynamic stabilizers and muscles comes into play. The glute muscles, deep hip rotators, other surrounding hip muscles, and core are essential for hip safety and performance.
An important note is that some athletes may have different bony morphology of their hips in which their femur or hip socket is more rotated forward (anteverted) or backward (retroverted). (17) In one situation, the gymnast may have lots of hip and toe rotation “out” but may not have any motion of “toes in.”
In another, the gymnast may naturally have lots of hip and toe rotation “in” but not have any moving “toes out.” A full movement evaluation and something known as a Craig’s test is the best way to practically assess if a gymnast may fall into one of these categories. (17) Adjunctive radiographic X-Rays or advanced medical imaging can also be helpful to see a boney congruency. Some may have a combination of dysplasia, hip socket rotations, femur rotation, and different pelvic alignments.
It is way beyond the scope of this text to breakdown all these different anatomical variants, but the reader must be aware of the simple fact that not all gymnast’s hips are the same. The gymnasts who are naturally mobile with very flexible hips are almost always the ones we see used as demonstrators for speaking presentations, clinics, videos online, and during other flexibility talks.
What is likely easy for that gymnast to do in a flexibility video online is because she has unique hips. That same drill may cause significant pain and limited motion in another gymnast who has very retroverted or less shallow hip joints.
Many gymnasts may be limited by their bony alignment, differently shaped hips, or less mobile capsule/ ligaments. It’s not always because they are not trying hard enough. Attempting to apply one general stretching exercise that a naturally mobile gymnast showed in a presentation may cause some serious problems for such a gymnast.
Trying to aggressively push through that bony or ligamentous limitation will only lead to pain and headaches for all involved. If someone is continuing to struggle with hip mobility, rather than just pushing more take a step back and consider this concept. Take them to a qualified medical professional for an assessment.
Why Do Gymnasts Lose Flexibility In The First Place?
Although there are conflicting viewpoints on this discussion, I have boiled my thoughts down to three main contributing factors as to why gymnasts may get stiff as they participate in gymnastics.
- Natural Growth – The most obvious reason is that the majority of people involved in gymnastics our young kids who have not yet fully matured. They typically are going to different degrees of growth spurts at different times, which is not perfectly associated in line with their chronological age. Different gymnasts grow at different times, and often have a few big spurts which are referred to as peak height velocity.During this time, the long bones of the femur, humerus, tibia, and other areas grow significantly faster than the muscular tissues can keep up with. This usually results in limited degrees of range of hip, shoulder, ankle, and wrist motion because the tendons, muscles, and the nerves that are being stretched are unable to keep pace. Many people see this in their athletes when they are struggling with flexibility, seem to have difficulties with skills because of longer limb abortions, and also feel a little bit awkward during their training. It comes an adjustment period, and there’s no great solution besides communication, modifying training as needed, consistent flexibility work, and making sure there is a really great balanced strength and conditioning program in place. Which leads to my second point
- Non-Balanced Strength Programs – At this point in my coaching and consulting gymnastics career, I have been fortunate to analyze hundreds of strength and conditioning programs from gyms across the world. This includes non-competitive, competitive, collegiate, and internationally elite teams. If there is one thing that I can consistently see is a large imbalance between training of specific muscle groups.Often times the quads and hip flexors are trained at a significantly higher proportion than the glutes and hamstrings as well as the external rotators of hip. In the upper body, the chest and lats are trained at a significantly higher proportion than the scapula and upper back, as well as the rotator cuff. This is a topic for a different time, but much of it stems from a stubborn culture that has not embraced external loading for gymnasts using kettlebells, dumbells, and barbells. Many of the basic movements using kettlebells or dumbells such as deadlifting, hip lifts, upper back rowing, and more train these muscle goups very well.

 When you combine this with a large amount of gymnastics specific shaping work that gymnast must do, you can easily create imbalances around the hip and shoulder joint. I find this is the main issue for those athletes that are struggling to make long-term progress inflexibility. Even worse, I fear that many gymnasts are being scolded for not having great flexibility when in fact the programs they are part of our treating those stability issues with a combination of not balance strength programs and not using scientific evidence for their flex ability methods. While there are definitely times when the athlete needs to put more effort into their flexibility or strength program, I think that many of us need to be more accountable in realizing that maybe we are giving to the problem.
When you combine this with a large amount of gymnastics specific shaping work that gymnast must do, you can easily create imbalances around the hip and shoulder joint. I find this is the main issue for those athletes that are struggling to make long-term progress inflexibility. Even worse, I fear that many gymnasts are being scolded for not having great flexibility when in fact the programs they are part of our treating those stability issues with a combination of not balance strength programs and not using scientific evidence for their flex ability methods. While there are definitely times when the athlete needs to put more effort into their flexibility or strength program, I think that many of us need to be more accountable in realizing that maybe we are giving to the problem. - Adaptations to Training – As I hinted at above, gymnastics requires a large degree of repetitive motions during training. Many skills, drills, and other technical training pieces require the exact same motions over and over to learn foundations. When you look at other sports, this turns out to the case for many young athletes. There are adaptations in muscular stiffness that are typically associated with repetitive training.Baseball players have been known to reduce their overhead flexibility and shoulder internal rotation due to muscular soft tissue stiffness the more they throw. Many runners report excessively stiff calves when they put on hundreds of miles of running over the course of a few years. Although it is not been shown any gymnastics study yet, I feel largely that just doing gymnastics will expose athletes to repetitive motions that create soft tissue stiffness. If not checked and readily worked on, they may create a loss of flexibility. In particular, the inner thighs, quads, and calf muscles of gymnasts are constantly used to maintain ‘good form’ but also sprint, hurdle, kick, and create shape changes. In the upper body, the lats, teres major, and packs are used repetitively to maintain proper shapes and also produce power on the equipment through shape-changing.
When you combine these three areas, along with the already discussed points about not having the best science behind flexibility methods to stress muscular tissue and spare joint capsules, it certainly makes sense why gymnasts may struggle with their flexibility. While puberty can make a big negative impact on flexibility, I feel that the cultural norm of gymnasts just automatically getting tighter as they age is overexaggerated. If better flexibility, strength, and soft tissue care was used, I feel a lot of this could be avoided.
Why Does Flexibility Training Work?
We must always remember that the structures that have the most opportunity for improvement, the active structures, should be the focus of flexibility training. These are the muscles themselves, to a small degree the tendons that connect muscles to bones, and largely the nervous system. The main way people approach increasing the flexibility of the active structures is through regular stretching.

Stretching has been around for decades in gymnastics as well as other sports. Many different thoughts and practices exist in daily gymnastics training. Static stretching, dynamic stretching, “active flexibility”, and PNF stretching (proprioceptive neuromuscular facilitation) are a few popular methods. Alongside this, there is a lot of confusion or misunderstandings about what happens when gymnasts stretch, why it helps increase range of motion, how much stretching is suggested as beneficial to improve flexibility, and how to make changes show up in skills.
I will take a few paragraphs to explain the current body of research on stretching, outlining some important studies that have been done. I will get a bit nerdy outlining the mechanisms, but then I will offer a “practical application” type summary for people to apply in training.
In its most basic form, stretching involves taking a muscle to its end range of motion, and holding the elongated state for a period of time. This can happen statically for a period of time (static stretching), with the use of momentum and holding of end range (dynamic or active stretching), or sometimes with muscle contractions and stretching together (PNF or proprioceptive neuromuscular facilitation).
Neurological vs Mechanical Effects of Stretching
A large body of research has emerged in the last decade outlining that regular stretching does increase range of motion over periods of 4-8 weeks, with both changes in the muscle tissue and changes in the nervous system as an underlying mechanism. (18-26)
It appears that a combination of mechanical factors (18, 25, 27-29), as well as neurological factors (18-21, 24, 25-26)), are reasons behind why regular stretching increases range of motion.
In terms of stretching induced neurological changes to the muscle tissue, the majority of the articles theorize that the main reasons behind this include
-
- A reduction in the threshold of stretch reflexes within muscles
- A reduction in the sensitivity of nerves that transmit signals of danger (nociceptors)
- A change within the brain related to perceived discomfort
- A possible increase in the levels of chemicals that are natural pain relievers, like enkephlin, within the body.
All of these mechanisms may be occurring as people stretch consistently over a long period of time. The main articles that support this are
-
- A paper by Weppler / Magnussun in 2010 (find it here https:// www.ncbi.nlm.nih.gov/pubmed/20075147)
- A paper by Konrad in 2014 (find it here https://www.ncbi.nlm. nih.gov/pubmed/24856792), and
- A paper by Ben / Harvey in 2010 (find it here https://www.ncbi.nlm.nih.gov/ pubmed/19497032)
With this being said, there are definitely studies that claim changes to the mechanical properties of the muscle, tendon, and junction between these structures change overtime with stretching. The majority of these articles theorize that the main reasons that stretching increases range of motion include
-
- A reduction in the amount of stiffness or compliance within muscles (viscoelasticity), although likely transient
- An increase in the length of contractile units within muscles (sarcomeregenesis) especially if eccentrics are used
- Increases in the water content, blood flow, and temperature within muscles acutely
The main articles that support this are
-
- A 2018 systematic review by Thomas et al ( https://www.ncbi.nlm.nih.gov/pubmed/29506306 )
- A 2012 paper by Zollner ( http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0045661 )
- A paper by Nakamura et al in 2015 ( https://www.ncbi.nlm.nih.gov/pubmed/25559637 )
Speaking beyond the research, I truly feel that both mechanical and neurological changes occur in muscles as well as tendons with prolonged stretching. This said, I believe the majority of the effects of stretching come through neurological means.
It’s my opinion that other aspects to physical preparation like strength or skill training, cause more structural changes to muscle tissue due to their higher force and volume nature. Especially in gymnasts, the changes in sensitivity of nerves that transmit pain, and also reductions in stretch reflexes likely are the main mechanisms.
I think that by using correct stretching consistently over time (not into excessive pain or passive tissue damage) combined with strength in full range of motion. eccentrics, or skill training, is mainly what causes changes in the muscle tissue itself.
The research definitely leans towards changes in the nervous system being the primary reason, especially in the short term. That said, there are certainly changes in muscle stiffness, as well as the length of a muscle, again when appropriately used stretching methods are used.
By this I mean those based on a proper assessment, that does not induce excessive pain, that has a consistency over intensity mindset, and uses stretching as once piece of a larger program for flexibility.
All of the studies that did show a change in range of motion from various techniques (static stretching, PNF type, more dynamic stretching) did not push the subjects into very extreme pain or use excessively long periods of stretching past 2 minutes.
In a research study by Ben and Harvey (9), thirty healthy adult individuals were compared to 30 people in a matched control group to see if regular hamstring stretching would
1) improve range of motion and
2) change the hamstring muscle extensibility.
It was found that thirty minutes of supervised hamstring stretching to the point of discomfort, five days per week for six weeks improved overall range of motion but did not increase the muscle extensibility. In simple terminology, it means that they did show an increase in the range of motion, but not due to a significant change in structural muscle tissue length. The researchers proposed that the change in the range of motion may have primarily come from increased tolerance to the discomfort of nerve fibers that detect stretch pain, as the fibers were becoming more desensitized. (10)
In another study by Konrad (10), twenty-five adult individuals were compared to twenty-four adult individuals in a control group to see if a six-week calf stretching program would
1) increase ankle range of motion and
2) change tissue properties of the calf muscle.
The twenty-five individuals in the experimental group stretched their calves in a standard protocol four sets of thirty-second calf stretches to the “point of tolerable discomfort”, five days per week, for six weeks. Wall ankle flexibility tests were used to measure the range of motion changes, and ultrasound imaging was used to look at the changes in the muscle tissue that relate to extensibility like passive resistive torque, muscle stiffness, tendon stiffness, fascicle length, and pentation angle.
Similar to the study above, it was found that while ankle range of motion did improve, there were no significant changes in the muscle extensibility outcomes that would indicate tissue change.
The authors concluded that
“the increased range of motion could not be explained by the structural changes in the muscle-tendon unit and was likely due to increased stretch tolerance possibly due to adaptation in nociceptive nerve endings.”
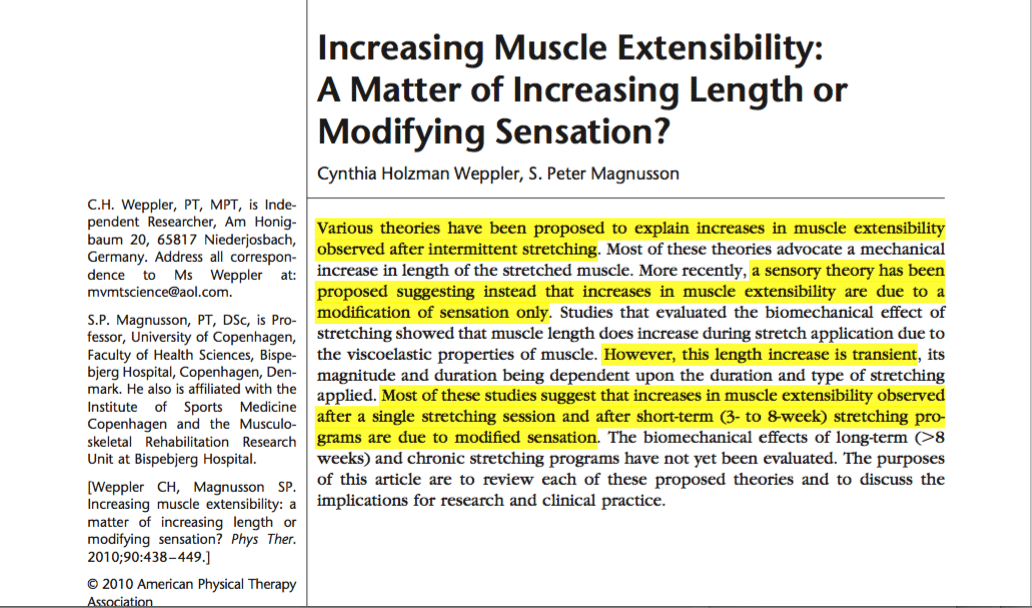
A very useful research review on this topic was performed by Weppler and Magnusson titled, “Increasing Muscle Extensibility: A Matter of Increasing Length or Modifying Sensation?” (18).
They review an abundance of research studies like the two noted above, dissecting the results and validity to offer thoughts on what stretching does to muscular tissue. Although I highly encourage people to review it and read the evidence for themselves, their thoughts follow in line with the ideas noted above related to changes in sensation or tolerance of stretching, rather than true muscle tissue changes. In their concluding paragraphs, they write,
“Traditionally, rehabilitation literature has attributed increases in muscle extensibility observed after stretching to a mechanical increase in muscle length. A growing body of research refutes these mechanical theories, suggesting instead that in subjects who are asymptomatic, increases in muscle extensibility observed immediately after a single stretching session, and after short-term (3-8 week) stretching regimes are predominantly due to modification in subject’s sensation.” (18)
Within all these studies, there were undoubtedly methodological issues that need to be considered. The subjects were adult, the stretching methods and outcomes may have some validity errors, and the difference in natural hypermobility or anatomy were not discussed. Gymnasts partake in stretching every day for months on end, so we can’t conclude that changes in muscle tissue over time are not occurring.
Other researchers combat these ideas and say that effects locally in the muscle like water hydration levels, changes in the viscoelasticity of muscles, and even interesting ideas down to stem cell changes within tendinous structures may be factors.
In a study by Zollner et al (17), the researchers looked more at changes in muscle tissue when chronic stretching was used in simulated animal models. These studies mainly look at chronic immobilization, like when people unfortunately need limb lengthening or tendon elongation procedures. Through very sophisticated mathematical models, they did show evidence of
“a mechanistic multiscale model for stretch-induced sarcomereogenesis, in which chronic muscle lengthening is characterized through a scalar valued internal variable, the serious sarcomere number.”
This would suggest that with significant immobilization or time spent in prolonged tension, sarcomeregensis may occur within the muscles. But, the timiing protocols for these studies were insanely more than and human does, so it’s likely not the main case for increases in muscle length. This is opposed to possible sarcomeregensis that may be induced from heavy loading eccentric movements.
Another study by Konrad et al (29) took thirty healthy men ages around 21 and subjected them to 4 sets of 30 second calf stretches. Half the group performed static stretches, while the other half performed “Hold Relax” stretching, a variety of PNF. They measured ankle range of motion and end range stiffness before and after these stretches. They ended up finding changes in range of motion for both groups, with more changes to the muscle tendon stiffness in the Hold Relax group. They concluded,
“ … that both Hold Relax Stretching and Static Stretching can increase end range of motion, which may be because of the decreases in muscle stiffness and modified stretch tolerance during the stretch application. In addition, compared with static stretching, hold relax stretching may have a great effect on the alteration of stretch tolerance rather than decrease in muscle stiffness.”
The important point here is that we must remember that changes in flexibility come about from slow, consistent, and patient application in training. Regularly using the correct flexibility exercises, skill progressions, and strength training assignments based on an individual movement assessment is by far the best way to ensure progress. Long term changes that have minimal injury risk do not tend to come from short-term, high intensity and high force methods often seen in gymnastics.
Why We Must Change Certain Stretches for Safety
Proper assessments and specific stretching methods must be used so that excessive strain on passive tissue like bones, ligaments, and joint capsules is avoided. Undue force to these passive structures becomes problematic over time as the high force of gymnastics can cause injury. In a sport like gymnastics, where very high forces are going through shoulder, hip, and spine joints at extreme ranges of motion, this level of force can quickly cause already mobile passive tissues to stretch out more.
I feel this naturally occurs over time but is amplified when stretching methods are misguided. When this acquired excess in joint laxity is paired with a lack of strength, lacking technical development, high repetition, and fatigue in not fully matured athletes, this may have a variety of negative consequences.
If the ligaments and joint capsules are already hypermobile, and have trouble dealing with high force, and then we add more laxity to them over time, we are likely asking for disaster regarding instability- based shoulder and hip injuries. (30-34). This is especially as recent research has shown that shoulder and hip injuries are one of the most common problems all gymnasts face. (25)
Much of the change in gymnastics to prevent these common injuries comes down to applying the research of anatomy as well as stretching and updated commonly used methods that may not fall in line with the literature. Remember we want to focus on the active muscular tissue, not the passive ligament or joint capsule tissue. We also do not want to cause excessive irritation of soft tissue through boney compression.
Common Shoulder Stretches of Concern
One example of this would be replacing a commonly used shoulder stretches for overhead handstand flexibility in training. These stretches below are seen daily in gymnastics.


As anatomical and biomechanical research in the shoulder outlines (1-5, 16) this end range overhead flexion and internal rotation position may create excessive pressure on certain shoulder ligaments over time. More specifically, the inferior glenohumeral ligament and capsule, as well as possible parts of the middle glenohumeral ligament and capsule. This end range compression and increase in capsular laxity over time may predispose shoulder instability, subacromial impingement of the rotator cuff or biceps tendon, and labral damage.
I do not mean to suggest that this shoulder stretch will cause injury in a gymnast and should never be used. For choreography or specific drills, this may be very appropriate when not pushed quickly to extreme ranges of motion. Skills like Shaposh releases for female gymnasts, Tipelts for male gymnasts, and other extreme overhead motion demands require this amount of mobility. When correctly applied certain stretches into this position can augment skill development.
However, my point is that in most cases with a gymnast (or many overhead athletes) we are looking to improve range of motion into this elevated position by improving the flexibility of specific soft tissues. Tissues most commonly targeted are the latissimus dorsi, teres major, and pec muscles. When this is the case, there may be a more optimal approach based on the anatomy of the shoulder joint. These common active structures limiting overhead shoulder flexibility we want to focus on making more mobile. If the exercises above are biasing stress on joint capsules and ligaments more so than the lat, teres major, and pec muscles, we should look for an alternative solution.
Another version of an overhead stretch, pictured below, is an example of the opposite. It uses either a floor bar or the other arm version to bias external rotation of the shoulder. The athlete is encouraged to round their upper back to create upper back flexion.

The thought process is that by following the anatomy of the shoulder joint and latissimus dorsi, teres major, and pec musculature 62-64, this version of an overhead flexibility drill biases stretching the soft tissue that needs attention and takes the pressure of the often already hypermobile shoulder ligaments.
This simple change in the stretch, along with follow up work, tends to make large progress in gymnasts who cannot progress in their overhead flexibility.
While on this note, there are a few stretches that really need to be advised against in gymnastics. I feel extreme passive stretching like these movements really serve little help in the process of safely getting shoulder flexibility.


While it is true that male gymnasts need extreme behind the back shoulder motion for pommel horse and pbars, I think there are much better ways to get it than being aggressive with behind the back stretch. Soft Tissue care, specific stretching, and eccentrics can help male gymnasts get where they need to be. I will dive into this more below.
Common Hip Stretches of Concern
Another typical example related to hip flexibility has to do with how arched a gymnast’s lower back is during hip flexor or quadriceps muscle stretching. A commonly seen stretch in gymnastics is when the lower back of an athlete is excessively arched, or the pelvis is excessively tipped forward as depicted below.

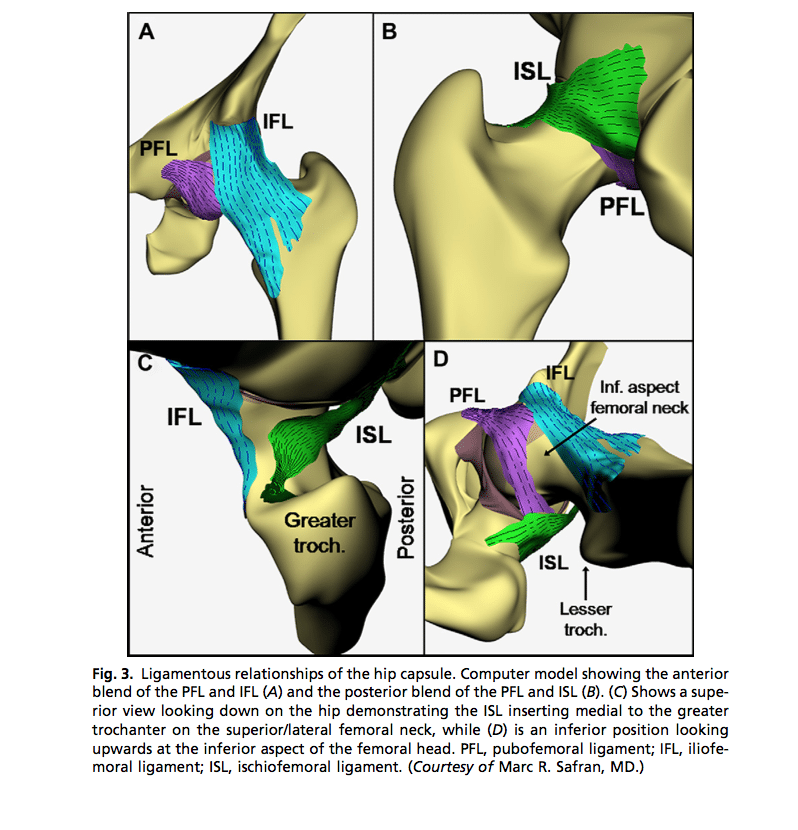
Similar to the shoulder, when you look at the anatomical and biomechanical science of the hip joint, hip ligaments, hip flexor and quadriceps muscle (5, 8-12, 17) the more the lower back is arched, or hips are tilted forward, the less these muscles may be biased in this stretching alignment. Instead, it may lead to the ligaments and joint capsules in the front or underside of the hips receiving more of the strain. These ligaments more specifically are the medial and lateral arms of the iliofemoral ligament and the pubofemoral ligament.
In parallel to the points made above, it is not that this stretch is inherently bad or dangerous for a gymnast. For choreography or specific drills this may be very appropriate. When used in the right context, it can augment the flexibility needed for advanced leaps or jumps, inbar skills, and tumbling mechanics.
The point is that targeting the soft tissue of the hip flexor and quad may be a more optimal approach. An alternative version based on anatomy would be to flatten the spine position as well as the pelvis, and then perform a similar stretch with core/glute engagement.


It does not look nearly as impressive of a motion, but it is very specific to the goal we are trying to achieve of affecting the active structures while minimizing excessive stress on the passive structures.
Frequently the complex research available suggests some minor changes during training. This can be seen with the examples above. Simple changes to choose types of stretching exercises that bias the correct structures of the hip or shoulder may make a notable difference in long-term flexibility and injury risk. It can be accomplished through an “addition by subtraction” type approach of using an alternative exercise or changing the alignment of certain common gymnastics stretches. The larger changes related to global training design, may be more involved.
As with the shoulder, I also feel that extreme hip stretching methods from a very high surface, or when a coach is pushing aggressively on a gymnast, have no place in our sport. I will talk more specifically about oversplits below, but I feel that the lack of education around this topic is why so many people are using aggressive methods. There is a much better way that is safer and has valid science behind it for support.
What About Static Stretching? Good or Bad? Helpful or Not?
I don’t want readers to think static stretching is bad, and that we shouldn’t do it. As the 2018 systematic review outlines (25), it may make a positive effect on range of motion when properly done. As it also highlights, there may be changes in the tissue over time, as well as neurological changes
There are times after a hard training session or light training day where I will have gymnasts perform a whole body soft tissue session and follow it up with more passive stretching. There is some research available that this assists in the perceived recovery process. (36-38)
However, the rationale for this is in a different context. In this setting, we are looking to ramp down the body and assist in recovery (known as facilitating parasympathetic tone). We are not aiming to ramp the body up for a training session or work hard to gain flexibility and train skills. In my mind, these are two different applications of static stretching or foam rolling and should be viewed as having different goals.
Speaking beyond the research on this idea, I think light soft tissue work and static stretching may have the most impact on blood flow or lymphatic drainage. It may help reverse the hypoxic or acidic environments that occur during challenging workouts. I will dive into the physiological thoughts on this in the recovery chapter. There is more support in the literature for the use of static and dynamic compression, but I think lighter recovery sessions of self-myofascial release, light stretching, or even light aerobic exercise are valuable tools alongside other methods.
Pausing for Practical Applications in Gymnastics Training – I know readers feel real overwhelmed probably. So here are some main take always to help.
- The issue is not with use of stretching. The issue is more about
- The lack of assessments being used before and after stretching
- The lack of flexibility exercises that target active muscular structures (muscles and tendons) over passive structures (ligaments and joint capsules)
- The lack of a “consistency over intensity” mindset that is supported by research, and also avoids aggressive techniques that may cause injury
- The lack of individuality and specificity being used based on a gymnast’s individual issue
- The lack of stretching being used as one small piece for the overall flexibility approach that carries changes in range of motion to actual skills
- The current body of research on stretching suggests that
- Changes in the nervous system are likely the main reason why stretching overtime increases range of motion (changing stretch reflex, changing perception of discomfort, desensitization of specific nerves)
- Changes in the muscle or tendon tissue itself also likely occur (change in number of sarcomeres, length of sarcomeres, amount of stiffness in muscle tissue)
- Static stretching in 30-60 seconds bouts, done 5 times per week, for a total time of 5 minutes per muscle group per week, to the appropriate limit of discomfort, is supported by a majority of research to be optimal for increasing range of motion. It was also outlined that total time spent stretching per week was more important than total time spent stretching per session. That article can be found below, but before readers jump to creating only static stretching circuits based on those parameters, please read the rest of this chapter.
Thomas E., Bianco A., Palma A. The Relation Between Stretching Typology and Stretching Duration: The Effects on Range of Motion. Int J Sports Med. 2018. [Epub ahead of print] Read this study here – https://www.ncbi.nlm.nih.gov/pubmed/29506306
- Other methods of stretching like active flexibility, and PNF stretching, are certainly effective for increasing range of motion.
- The most effective approach to increasing flexibility may be when stretching is used with proper assessments, consistency in stretching, follow up control work, strength programing including eccentric training and proper volume / fatigue management for athletes.
Sands and Mcneal have a few fantastic chapters on flexibility in recent Strength and Conditioning text books (39-40). It is worth noting that both authors have extensive experience in elite level gymnastics, spending the majority of their career researching gymnastics biomechanics, injuries, and sports performance. I am incredibly grateful for all the research they have conducted.
Through their chapters, the researchers outline that flexibility training must be viewed in a broader context outside of only aiming to increase joint range of motion. They explain that the short-term effects often seen from stretching must be supported by other qualities of athleticism. They accurately outline that areas like muscular strength and joint control must be trained in parallel with stretching.
They outline, as do many other great researchers, that correctly performed stretching bouts of 10- 30s that move to tolerable discomfort can be effective. They also outline that longer durations of stretching (say up to 2 minutes per stretch) show “diminishing returns”. They also echo the research covered already that emphasis how overly aggressive or excessive stretching duration can “possibly have damaging effects on connective tissue”(39)
Is Foam Rolling A Waste of Time?
“Self-soft tissue work” refers to using foam rollers, lacrosse balls, tennis balls, or other implements to help massage different muscular areas of the body. It has all become wildly popular in the last five years, and it’s starting to show up much more in the gymnastics community. I think that daily soft tissue care is one important piece of the puzzle.

I feel gymnasts should be doing regular soft tissue care routine to combat excessive stiffness that may negatively impact flexibility. Some research has suggested it can also be helpful to reduce perceived muscle soreness, enhance blood flow, and make an impact in recovery (41-43) I encourage all athletes that I work with to do some form of light, soft tissue prep before every workout. This becomes more important as the athlete gets older, starts training higher-level skills, or are spending more hours per week in the gym.
The body of research regarding foam rolling and manual therapy or massage is a bit confusing regarding the theoretical mechanisms. The most popular thought process is that we are affecting resting muscle tone, possibly increasing blood flow, perhaps changing the amount of water hydration level within the muscle or are offering a competitive neurological stimulus for muscle soreness. As mentioned above, the research mainly leans towards changes in perceived discomfort through neurological mechanisms over changes to muscle tissue, especially in the short term (41-42).
Most healthcare providers that I have talked with feel the major benefits of self-soft tissue work are increasing blood flow and allowing muscle relaxation. Given the material I have read, this has been my main thought process as well.
Conflicting Research on Foam Rolling and Other Soft Tissue Care
There has been conflicting research on the long-lasting changes in range of motion from various stretching methods as well as self-soft tissue work. There appear to be short-term changes in range of motion, but often does not stick around too long without follow up strength work or consistent practice of flexibility.
The systematic review by Chris Beardsley and Jakob Skarabot in 2015 outlines (41) that when analyzing various studies, foam roller use “appears to lead to acute increases in flexibility in the majority of investigations” despite a few studies not reporting acute changes in the range of motion following forms of foam roller use.
Conflicting results may have to do with the types of tools used, the pressures used, the duration of treatment, and technique or instructions were given to study participants. Importantly enough, following a review of the literature, it was outlined that the combination of appropriate self-myofascial release and targeted static stretching may yield the most beneficial gains to acute changes in flexibility.
Due to the outlined research effects of foam rolling, stick or other forms of self-massage, I regularly recommend it as a piece of a gymnast’s flexibility training. It by no means is the perfect solution, but when based on a movement assessment and used with other strategies, self-myofascial release can be very beneficial.
I typically have gymnasts perform moderate pressure that does not cause pain, for 10-30 seconds per muscle group, away from bony areas. This is because a large body of manual therapy and self-soft tissue work does not recommend very intense/painful pressure, or extremely long bouts of foam rolling are needed to gain the positive benefits. (41-42, 44-45)
In my experience, excessive force, excessive duration, and the incorrect placement of a foam roller or stick massager can have opposite effects. It’s very important that both coaches, gymnasts, and medical providers understand this research to not see negative results from these tools, or worse cause unintended damage.
I know some coaches worry that excessive static stretching or foam rolling before training may negatively impact strength or power output, based on concerns or some research findings. (46-48)
However, more recent research has supported the idea that foam rolling and properly designed dynamic warm-ups prior to training appear to have no significant negative effects on performance, may enhance it, and also positively impact the range of motion in various muscle groups (49-50). From looking at self- myofascial release and manual therapy literature reviews, this is thought to be through changes in perceived soreness, neurological relaxation, and possibly blood flow / water content shifting within the muscle.
Again, as presented by Beardsley and Skarbot,
“Self-Myofascial release does not appear to impede athletic performance acutely or in the short term. The average quality of studies included in this section of the review was slightly higher than the average qualities of the studies in the review overall. In all cases except two, (Janot et al., 2013; Peacock et al., 2014) there were no changes in performance measures following any of the SMFR protocols used”
From all the science I have read, and conversations I have had with medical professionals on stretching or self-myofascial work, when correctly applied the positives effects of foam rolling on performance largely outweigh the negatives. In support of this, my experiences working with hundreds of gymnasts to improve flexibility also supports the use of regular stretching and foam rolling for the range of motion, perceived soreness, and perceived recovery, with minimal negative impacts on performance. I recommend these tools be used alongside full dynamic warm-ups and technical drills commonly seen in gymnastics.
I want to emphasize that proper stretching and soft tissue work is not the only method to improve flexibility and performance for gymnasts. It is only one piece of the puzzle that must be used in combination with movement assessments, strength work, technique work, consistent practice, and periodization programs that calculate work to rest ratios. These topics tend to be what I write and lecture about most because they are often underrepresented or misunderstood in gymnastics. The science must be blended with expert coaching opinion and consistency in training.
Many of the gymnasts I coach or treat for injuries report that light, soft tissue work makes them feel more warmed up and helps to reduce perceived muscle soreness. They also claim it helps following hard workouts or on light training days to recover. Many also claim that it helps them move in a larger range of motion with less discomfort before starting their practice. A few very inflexible gymnasts that I have worked with also displayed improvements in hip or shoulder range of motion over time when they used soft tissue work combined with proper stretching/strength programs.
As a healthcare provider, I regularly perform manual therapy to help with injuries based off a full medical assessment. Just as with the warm-up concept above, it is only one piece of the bigger puzzle to increasing shoulder or hip flexibility long term. I can often see an appreciable change in the range of motion within only a few sessions, pending that gymnasts are dedicated to the follow-up a home program.
Many gymnasts will continue to see me in the competitive season for maintenance care, as they can notice how adaptively stiff they become through high volume of training or competing. My mentors have outlined that this was a crucial part of their work in professional-level sports through the competitive season, so I have adopted it into my practice with gymnasts. These are just anecdotal experiences, but they are in line with what the literature outlines.
I agree that research is conflicting on the theoretical mechanisms and effects of soft tissue work, but it seems to be making some positive effect that supports its use. I know there is a large spectrum of positive or negative views on soft tissue work. For me, it takes a minimal amount of time and does not seem to have too many negative effects when correctly implemented. I view it as a tool to open the door for gymnasts to then perform strength, technique, and control work for gymnastics skills.
My best recommendation is that people become more familiar with the research, practice, and use of self-soft tissue work. They can also partner with healthcare providers who are versed in this information to either to teach in-services to their staff or teach the gymnasts themselves.
Why Movement Assessments Are Key For Finding The Root Problem
Moving past all this background information, it’s time to talk about what actually causes a gymnast’s arms not to go overhead in a handstand, a gymnast’s legs to not go into a full split, or a gymnast’s arms to not go behind their body for pommel horse swings. Many medical assessments can be used to determine why a gymnast’s hip, shoulder or spine may not have the range of motion needed to achieve a full handstand, split, or bridge.
The reality of the human body is that there are hundreds of factors related to anatomy that can influence a gymnast’s level of flexibility. There are many possible reasons for why a gymnast can or cannot move their hips into a full split position or move their shoulders overhead into a full handstand position.
Without a proper movement assessment being done first, the application of regular stretching and other flexibility exercises may fall short of revealing progress. Even worse, if the underlying cause of limited flexibility is not found, we could be causing more problems to come up down the road regarding injury.

As mentioned, the important take away here is to focus on things we can change, like the muscles themselves. Other things are beyond the realm of changing unless you have a medical background. The way someone’s hips or shoulders are shaped, unique rotations of bones, certain anatomical variations, or issues along the entire body chain, can all have a substantial impact on the amount of flexibility a gymnast can display during skills.
It is not always about the length of the muscle at one spot like the hip or shoulder that makes everything goes right. The reality of the situation is that a variety of muscles around the hip or shoulder could be the culprit.
Alongside this, strength deficits, limited full range control, technique issues, fatigue, or adjacent areas of the body may be the reason behind an apparent lack of flexibility. These issues are commonly overlooked as culprits to why a gymnast struggles in this area of gymnastics.
Without the ability to assess these various factors, it can be very challenging to make progress in flexibility. I urge people to not automatically push splits or pull shoulders open when they see a gymnast with limited range of motion.
Components of Splits and Handstand Flexibility
Everyone in gymnastics should understand that there are many subcomponents of split, overhead handstand, or behind the back patterns that must be worked on. For example:
Right/Left Leg Splits –
- Underlying bony hip anatomy (retro or ante verted femur or acetabulum, depth of hip sockets, boney leg length discrepancy)
- Core control and strength
- Front leg hamstring extensibility
- Front leg groin extensibility
- Front leg calf extensibility
- Back leg hip flexor extensibility
- Back leg groin extensibility
- Back leg quad extensibility
- Glute and deep hip rotator strength on the front and back leg
- Neural tension in sciatic, femoral, piriformis, and quadratus femoris nerve
- Motor control in full range of motion
- Lack of protective guarding against tissue injury
- Coordinative dynamic stability of hip and core muscles
Overhead Shoulder Flexibility
- Underlying bony shoulder anatomy (retro or anteverted humerus or glenoid, depth of shoulder sockets)
- Core control and strength
- Latissimus dorsi muscle extensibility
- Teres major muscle extensibility
- Pectoralis major and minor muscle extensibility
- Tricep muscle extensibility
- Thoracic spine extension and rotation joint mobility
- Lower cervical retraction and rotation mobility
- Rotator cuff and scapular strength
- Forearm and wrist extension mobility for proper stacking
- Thoracic outlet neural compression and extensibility
- Motor control in full range of motion
- Lack of protective guarding against tissue injury
- Coordinative dynamic stability of rotator cuff, scapular, and larger prime mover muscles
I do not mention this long list to make people feel uneducated. I suggest these to outline the complexity of the human body, in hopes that people are more cautious in some flexibility decisions they make.
It can be overwhelming if you are not familiar with it. The analogy I use with people from a coaching background is to compare it to the giant swing and the necessary components to complete the skill. For a giant to be technically sound, many sub components must be present.
Proper Giant –
- Physical preparation of basic shaping
- The ability to create whole body tension that optimizes storing energy within the bar bending
- Proper kipping mechanics
- Proper cast handstand mechanics
- Proper hollow falling shape into tap
- Tapping mechanics of hollow – arch – kicking
- Correct timing of shape changing
- Finishing hollow position to carry momentum over the bar Enough repetitions to maintain technique memory
Just as we must reverse engineer each of these technical issues to why a gymnast is unable to make a giant over, we must take the same approach to flexibility training. We must educate ourselves on what components go into a full handstand or split positions, then be able to reverse engineer why a gymnast is struggling.
Simply doing more splits or pulling shoulders open with stretches that are a bit extreme will likely not get to the cause of the issue. I have found that many of the traditional general stretches we use as go to methods for increasing flexibility do not have proper assessments preceding them or may not have anatomical considerations in mind. Due to this, they may not be biasing the proper muscular tissue intended and as a result may show limited effectiveness.
I’m not saying all the stretches or flexibility approaches we use must be discontinued because they are dangerous. I’m just saying there are many factors to consider and that there may be a more optimal approach to take. I see many shoulder stretches, and hip stretches that I feel are putting a crazy amount of stress on joint capsules and ligaments. I do not feel they working as intended to address the true problem of muscular soft tissue stiffness.
By understanding these concepts, people in the gymnastics community can save a significant amount of time while also reducing the risk of injury during flexibility training. Approaching this goes back to the chapter on why an interdisciplinary approach to the future of gymnastics is needed. There are screening tools that coaches can use to assess these issues, in addition to many great assessments that medical providers can use to break down problems. This is where we will go next.
Not Feeding The Fire with Strength and Physical Preparation
With this concept of overuse muscular stiffness in mind, I want to pause for a critical point. I find many gymnasts who have shoulder injuries or are struggling with flexibility display significant strength deficits within their upper back and scapular area. The muscles of the shoulder blade and upper back are often not nearly as developed as the chest and underarm muscles mentioned above.
It is common to see many gymnastics strength programs that train a high volume of pull-ups, leg lifts, rope climbs, and push-ups. These programs often do not have the same volume of upper back strength work such as feet elevated horizontal rows, renegade rows, band pull apart, or basic rotator cuff strengthening. I believe addressing this common imbalance in strength volume is a key contributing factor for seeing long-term shoulder flexibility gains and reducing overuse injuries related to the shoulder joint.

Exercise selection, strength program balance, and athlete individuality also have a significant impact on limited progress in flexibility. If a gymnast is known for having “tight shoulders” that limits their handstand and swinging skills, why are we continuing to have that athlete do a high volume of pull- ups, rope climbs, push-ups, and leg lifts? Doing a high volume of these movements may create ongoing stiffness in these areas, and as a result further contribute to the persistent loss of overhead mobility.
A better option would be first to modify the amount of pull up or rope climb volume these athletes do, and instead replace those exercises with more horizontal pulling type motions to help create balance. Also adding in regular soft tissue work and mobility drills would be very important. This will help them continue to get the strength training effect but won’t continue to perpetuate their overhead mobility issue. In the long term, the increased strength of the upper back and follow up technique work will solidify the flexibility gains made.
The same argument can be made for the hips of gymnasts. Many gymnasts struggle with excessively tight hip flexors, inner thighs, and quads. They also are usually subject to 100s of squats, squat jumps, and leg tigthening exercises per week. It’s not that these are bad, but there needs to be equal amount of hamstring, glute, and deep hip external rotator work as well.

Many gymnasts with stiff hips could benefit from a bit less squatting and jumping, and repace those exercises with glute and hamstring work. Doing slider crawls are a great core training replacement to reduce some of the leg lifts that may be creating ongoing headaches with limited split flexibility.
What About Warm Ups and Cool Downs?
Warm ups and cool downs are another common topic that comes up when discussing flexibility. Many people want to know what the best approach is, either static or dynamic, if they should be aiming to increase range of motion, what are the best drills, and so on. For me, I think the discussion must start with the intended goal of the flexibility work. There are some times when we are aiming to just get the body going, and other times when we are looking to truley increase joint range of motion. I view the different goals fo flexibility in this light,
- Warm Up – Prepare the available flexibility athletes have, and prepare the body for training
- Flexibility Circuits – Look to increase joint flexibility or mobility through step by step circuits (more below)
- Cool Down – Help the body slowly ramp down into recovery mdoe following a hard training session. Typically not a time to increase joint motion, as the body is usually in a very high-stress state and has just taken a lot of training volume
In my mind, the warm-up should not really be the main time we are looking to make massive changes in flexibility. Warm-ups are typically best looked at as a time when you can prepare the available joint range of motion that a gymnast has. There are usually large groups of people warming up, a limited amount of space, and a limited amount of time. Also, you must remember that immediately following the warm-up genetically go to an event has very high forces. We do not want to excessively relax the muscular tissue and increase lots of joint motion before we then subject them to extremely high forces. For that reason, I typically approach the warm-up is getting the body ready for the training session.
Although there is a lot of research and textbook chapters written on these concepts (38-40), I have found that a multi step warm-up seems to be the best approach for this goal. I recommend athletes start with light soft tissue prep or individual areas of focus before practice, then do a joint based preparation, followed by some light cardio to increase metabolic temperature and heart rate, and then do a full dynamic warm-up. Following a full-bodied dynamic warm-up, athletes can then do some core basics, jumping and landing basics, handstand or other gymnastic specific prep work, and then progress naturally to their first about. You can see a video of our entire warm up here
As far as specific flexibility circuits, those I feel are the best times to truly make positive increases in joint flexibility. I will cover those in-depth below.
Are Oversplits Bad for Gymnasts?
After having various conversations about flexibility with people in the gymnastics community, the safety of training over splits is typically the biggest question.

In the most basic sense, I don’t think oversplits are inherently “bad for gymnasts.” I think the more accurate way to describe them is that over splits may be bad for a particular gymnast at that moment in time. Some degree of abnormal hip bone motion may be needed for success in aesthetic sports. I think there are not yet studied boney adaptations to the hip joints of gymnasts when correctly performed and consistent stretching occurs in younger years. I have this theory based on the changes in boney rotation that baseball players exhibit from throwing when younger. This is a central concept to the work my mentors Mike Reinold and Lenny Macrina teach their patients about, due to how much it changes their mobility.
For example, this research study (https://www.ncbi.nlm.nih.gov/pubmed/26944667) recently looked at x-rays from professional ballet dancers during full straddle splits. They found that to achieve this full straddle split position; there was evidence of micro subluxation in the hip joints. This means the hip bone was slightly migrating out of the hip socket to reach such large ranges of motion.
This finding isn’t inherently dangerous, or good as research always has its internal issues. More research is needed, but this concept of natural boney adaptations in gymnasts is a central idea I feel will emerge in years to come. The research in ballet dancers made me reconsider what must happen at the hip joint go to achieve such large ranges of motion needed for oversplits. Although it’s purely anecdotal, I have consulted with cases where x rays show a very similar phenomenon in gymnasts doing oversplits while getting hip xrays.
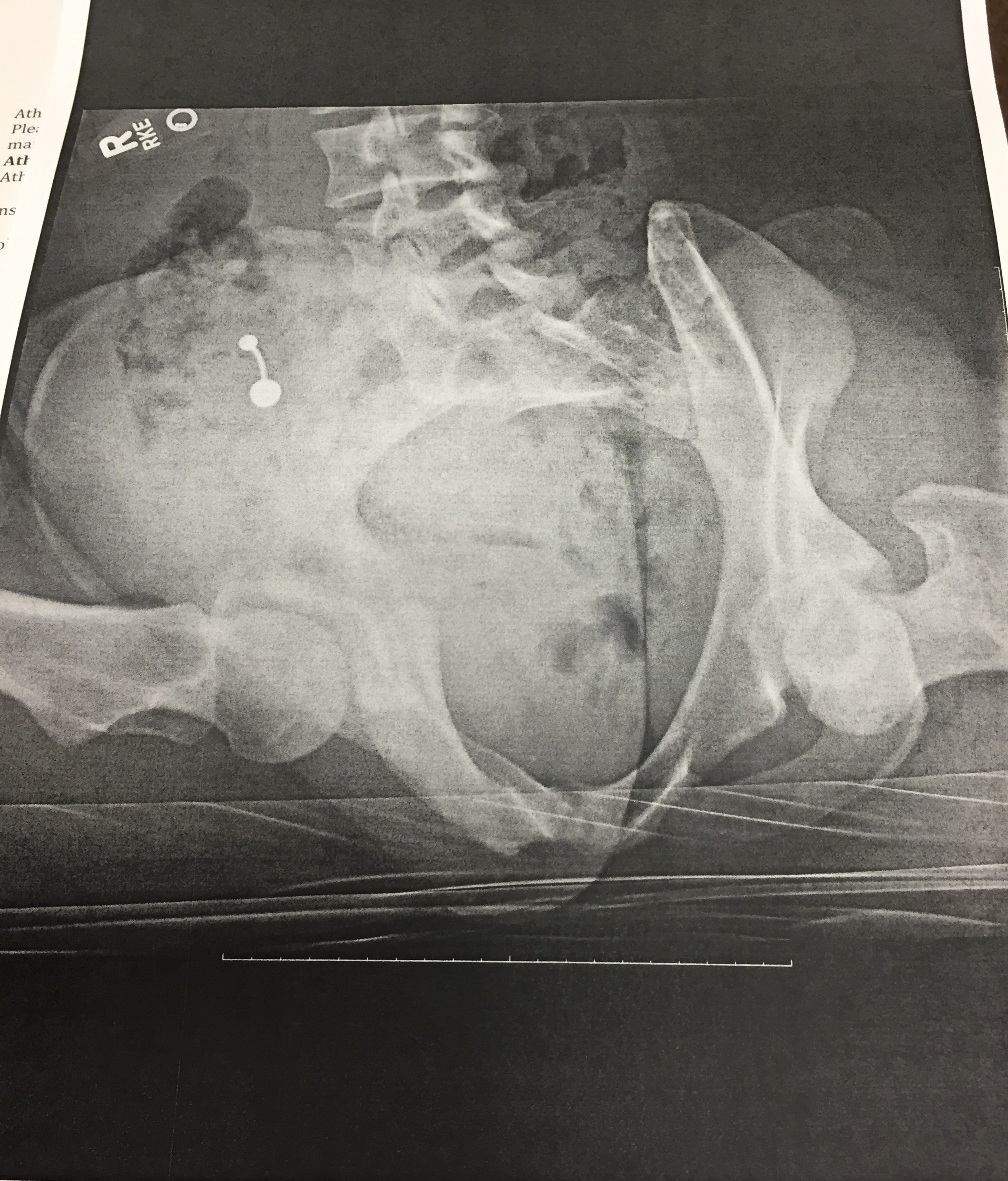
Keeping this in mind, we need to seriously consider that gymnasts have open growth plates and can suffer from ischial apophysitis or growth plate stress fractures if we blindly force split motion.
Forcing a split down into extreme ranges of an oversplit without a proper assessment behind it, asking a gymnast to perform over splits when they are not even close to a split on flat ground, or blindly pushing someone down just to be tough, is most definitely dangerous.
The main reason as mentioned above is because the “stretch” pain reported may be coming from a few overlapping body structures, some we should be aiming to target (muscles, fascial tissue, some tendinous) and some we should not be (bony joints, ligaments, capsules, labrums, etc.).
Without an in-depth knowledge of medical assessments, it is difficult to know why a gymnast may be limited in their split and what structure is referring discomfort during flexibility training. Being able to achieve a full over split, or even a regular full split for that matter requires many things to be going well from a movement point of view.
This is where things start to get important. Some of the movement-based components that must go right to perform over splits include:
- A naturally hypermobile type genetic structure, and ‘shallower’ hip joints (acetabular dysplasia)
- Proper spinal control, alignment and awareness that does not stress the lower back or hip joints excessively
- Adequate muscle length in the hip flexors, quads, hamstrings, and groin
- Adequate muscle strength in the core, glutes, deep hip stabilizers, and rotator muscles to safely support the hip joint
- Adequate full range control and strength for the central nervous system to allow leg motion to occur safely
- Consistent training and regular use of newly acquired motion to transfer motion to skills in the long-term
- Proper mental and psychological developmental/maturity of the athlete to actively be engaged in the training, know normal versus abnormal levels of discomfort and consistently work to seeing progress
As you can see, there are quite a few things that can limit why someone cannot do a full split or over a split. At face value, they can all appear as someone who is “tight” or “unflexible.” Which leads me to my most important point of this section:
Splits and over splits should not be viewed as an inherent thing a gymnast has or doesn’t have.
It should be considered to be a skill with many pieces that must be broken down to achieve success. Using proper movement assessments, understanding the anatomy, and a “consistency over intensity” mindset is what will reduce injury risk and increase gymnastics performance.
Now after saying that over split training is not inherently dangerous or going to create injury automatically, we all must realize there are severe consequences for not approaching split flexibility correctly. I strongly feel that gymnasts must “earn the right” to do over splits and must be mature enough to do them safely.
Simply throwing a bunch of random flexibility drills you recently saw at a clinic or on a video (I’m majorly guilty of this one) is a quick way to ask for complaints of hip pain. Also, aggressively pushing a gymnast down in a split or not taking the time to break down why someone is limited can also lead to serious injuries.
Before you apply new flexibility ideas, take a step back and consider the scientific rationale behind them. Also, think how they apply to the gymnast’s skill profile. Then brainstorm how to divide out the group of gymnasts who may or may not fit, and who may need an alternative exercise based on their issues.
Recently many gymnasts are reporting to have “hip flexor strains” that they push through. However, they may have a more serious underlying issue such as ligament, capsule, the joint or labral damage that are frankly a big deal.
Many great studies have outlined how hip ligaments and labrum may get strained at very end ranges that are unprotected or repetitively subjected to high force (as seen in several gymnastics skills). I will say take these research studies with a grain of salt due to their methods, smaller sizes, and sometimes using cadavers as subjects.
It’s not that we want to freak out every time someone is reporting discomfort in a split. However, we need to understand that forcefully pushing oversplits, not being open to learning basic anatomy, or ignoring serious pain complaints from gymnasts is not tolerable.
A blind approach to gymnastics flexibility training can cause serious hip injuries as the current medical research field has demonstrated. Labral tears may progress to requiring surgical repair and putting an athlete out of training for months or even career-ending. Long-standing hip micro instability is another concern that may be created without the proper training approach. If you are more curious about learning the medical side of hip injuries in hyper-flexible athletes, I highly recommend reading these articles.
- Skendzel, et al. The Approach to the Evaluation and Surgical Treatment of Mechanical Hip Pain in the Young Patient. J Bone Joint Surg Am, 2013 Sep 18; 95 (18): e133
- Dumount GD. Hip Instability: Current Concepts and Treatment. Clinics in Sports Medicine July 2016Volume 35, Issue 3, Pages 435-447
- Weber, et al. The Hyperflexible Hip Managing Hip Pain in the Dancer and Gymnast. Sports Health: A Multidisciplinary Approach April 23, 2014
- Shibata, K.R., Matsuda, S. & Safran, M.R. Is there a distinct pattern to the acetabular labrum and articular cartilage damage in the non-dysplastic hip with instability? Knee Surg Sports Traumatol Arthrosc (2016). doi:10.1007/s00167-016-4342-4
- Kalisvaart MM, Safran MR. Microinstability of the hip-it does exist: etiology, diagnosis, and treatment. J Hip Preserv Surg (2015) 2 (2):123-135.doi: 10.1093/jhps/hnv017
Sadly, many young gymnasts are requiring hip surgery, or are retiring due to hip injuries of this nature. Part of this may be inevitable for high-level gymnastics, but we should be doing anything we can to reduce risk given the scientific information and coaching expertise available.
Are Ankle Weights Dangerous?
The next most common question people ask me in this discussion is, “what about ankle weights, are those bad for gymnasts hips?”

The biggest concern I have with the use of ankle weights is related to two concepts of hip impingement and hip instability. I feel this issue comes up during fast dynamic movements like jumps, kicking drills, leaping, running, men’s pommel work, and so on. Anyone who wants a fantastic read and more elaborate background on these concepts again I recommend you read this article: “The The Hyperflexibile Hip: Managing Hip Pain In Gymnasts and Dancers“. I will try to provide simple explanations and also include graphics for the concepts.
Hip impingement refers to the femur bone and pelvic bones make contact with each other at extreme ranges of motion, most times causing pain and possibly damaging the soft tissue in between. Hip instability refers to the hip moving into to those same end ranges of motion without strength/control, causing the head of the femur to partially slide out of the hip socket. These two things often happen together in very flexible gymnasts, theoretically as the contact of the femur on the pelvis creates a “fulcrum” type point for the head of the femur to lever against contributing instability.
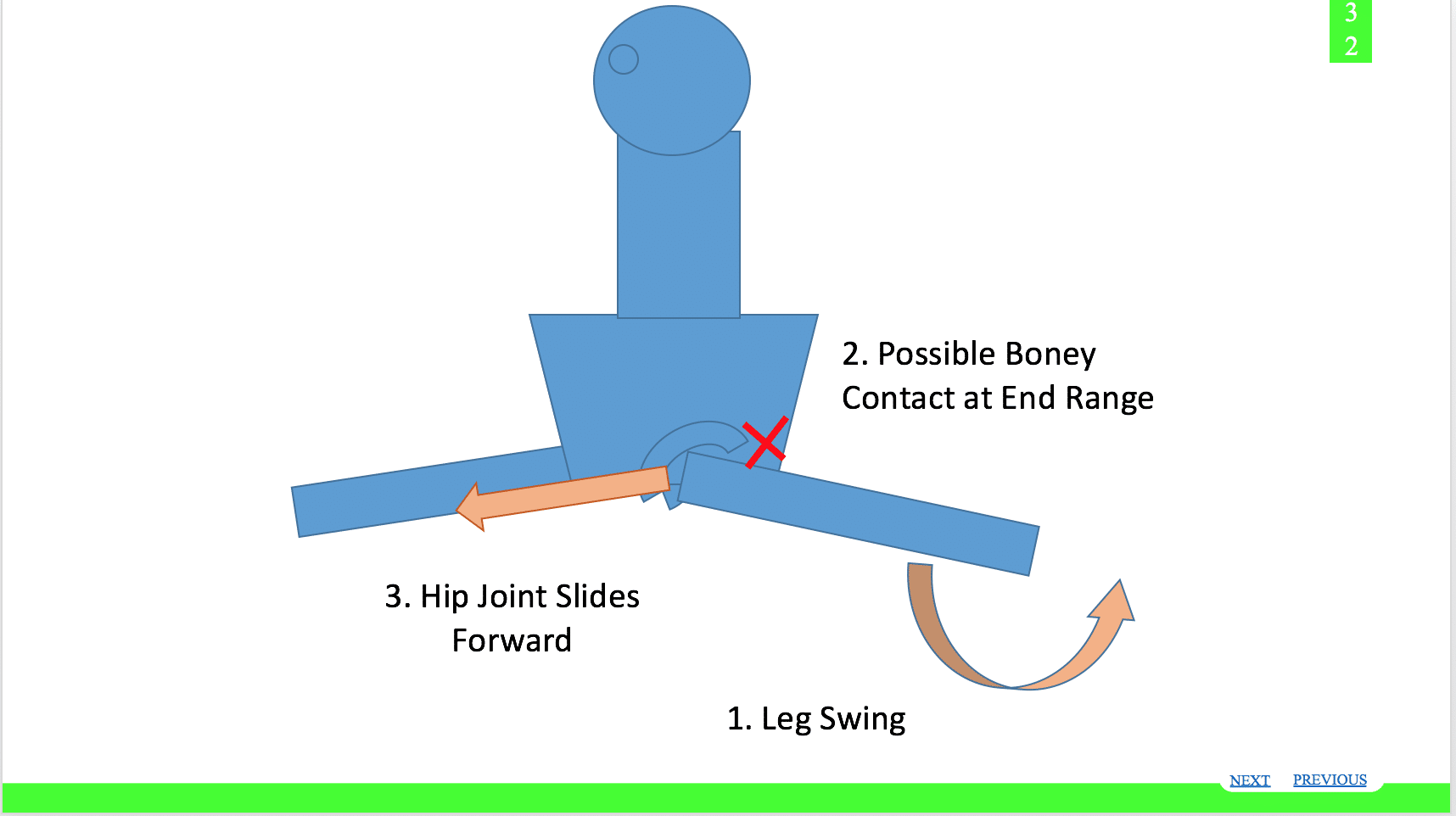
Moving from here, I will start covering specific joints and ways to help. It will be much less explanation, and more just videos and examples on how to help.
It may cause irritation to the impinged tissue, but also excessive strain to soft tissue and the hip ligaments/capsule that are being stretched with the instability.
- This can happen with hip flexing movements (think front leg high kick or leap) as the front of the femur bone makes contact with the front of the pelvis (impingement) and then the contact acts as a fulcrum for the femoral head to slide out the back of the hip joint (instability).
- This can also happen with hip extending movements (think back leg kick or leap) as the back of the femur bone makes contact with the back and outside of the pelvis (impingement) and then the contact acts as a fulcrum for the femoral head to slide out the front of the hip joint (instability).
Now let me tie this into why I no longer use of ankle weights. The ankle joint is very far from the hip socket. The farther the load is away from the joint, the more force it will have on it. It’s my opinion that using ankle weights under high speed (like in leaps, jumps, leg kicks, running, gymnastics skills/drills) will be very challenging for gymnasts to control due to the long weighted lever arm. Unfortunately, I feel the load at the end of the limb may contribute more to the forceful hip impingement, and also contribute more to the “fulcrum” based instability/subluxation stretching the soft tissue and possibly irritating the hip joint.

I think this is especially true in those with natural hyperflexible hip joints who are not fully developed and lack hip strength. This may be one reason why so many gymnasts say their hips hurt when they do jumping drills, running, or skills with ankle weights on. Again, these are just my thoughts. To really see if it is true I would need a dynamic MRI machine, a super slow motion high def camera, and someone way more technologically savvy than me (anyone want to put in donations?).
Secondly, I have also found that many gymnasts have significantly increased passive range of motion due to naturally laxity, but have a notable lack of active control for their full hip ranges. This is especially true when not allowing compensation from other body parts or excessive swinging for momentum. They often struggle quite a bit to lift their legs even against gravity alone. In this situation, if the gymnast can not access their full range of motion against gravity alone, I see no justification for adding additional ankle weight resistance and allowing swinging momentum to reach the desired end range of motion. I feel this may not only foster more compensation, but it may create overload based injuries to muscles and tendons in conjunction with the principles above.
Third, on an even geekier motor control point I think the use of external loading far away at the ankle joint greatly distorts the movement pattern the brain is trying to adopt neurologically. In simpler terms, I think that ankle weights make the skill very different compared to just the weight of the leg, and don’t accurately represent/have transferred to nonweighted leaps. Many people say how easy their jumps and skills feel after taking them off, but I think this is a short-lived neurological “trick” that may not have the best long term carry over.
Now please don’t take this as me not being a fan of external loading for gymnasts, as I am a fan of that when properly used (see article here). So, what are some solutions to maybe moving away from aggressive stretching/ankle weights but still developing beast like leaps/jumps? I’m glad you asked! Let’s dive into some safer and more science-supported methods.
How to Help – Working In Complexes vs Just Stretching
Given all of this, instead of doing twenty to thirty minutes of only stretching exercises, I now feel working in a complex type format is the most beneficial approach. I have found that it not only can yield quick changes in flexibility, but it can also make longer-lasting changes that show up in gymnastics skills.
The traditional model of gymnastics typically involves twenty to thirty-minute time periods where static stretches are held, active flexibility drills are done, or specific exercises are repeatedly done in high volume to gain range of motion. I did this for a decade as a gymnast, and for the first five years I was coaching. Knowing what I do now from all of the above research, I have mostly moved away from this approach of only using stretching to improve flexibility. This is true both in training and in our medical clinic.
One of the most effective methods that I have come up with to increase flexibility, make changes stick, and not risk injury with aggressive stretching techniques is to work in complexes rather than performing only static or dynamic stretching.

While I think these longer static or active flexibility circuits do have some value (and this is supported by research when used properly), the abundance of research outside of just the literature on stretching suggests a more optimal approach. Although these traditional training methods can yield short-term benefits and may help increase an athlete’s awareness of body position, problems clearly exist with this model.
For one, proper movement assessments are rarely done before these large flexibility sessions. Often the specificity or individuality of specific exercises lacks as a result.
Second, most times there are a lack of pre and post-tests (line splits, checking objective shoulder flexibility screen against a wall) to see if what is being used for exercises is effective. People assume that progress is being made, rather than having some comparative baseline for observing changes. If a training strategy is not yielding results over a few days or weeks, we must change and reevaluate our methodology.
And lastly, passive or active flexibility exercises alone will not have a substantial impact on the nervous system to change movement, build strength, or correct technique. This approach may lead to a limited transference to actual skills. It may help improve range of motion acutely, but it will not change movement in a gymnastics skill-specific manner. Despite our best efforts we may continue to see cast handstands that lack open shoulders, leaps that do not have larger angles, and parallel bar swings that lack a large front swing.
Due to these reasons and the research I have read about the human body, there will likely be a very limited long-term change in flexibility that change gymnastics skills. We must remember Dr. Sand’s advice to view flexibility not as a static quality, but as a dynamic quality that incorporates strength, power, and control.
I feel to see a notable lasting change in the range of motion that shows up in gymnastics skills, we have to approach the entire movement system with our mobility work, and not just aim to improve the range of motion seen. As I mentioned above, research does support specific stretching and soft tissue work, but as one piece to a larger program. This is why I now mainly approach flexibility in larger complexes.
A complex typically includes these steps (I will offer links to videos below)
Pre Test Screen
Splits on line, back to wall overhead shoulder motion, crab position for a male gymnast to assess parallel bars and pommel flexibility Self-Soft Tissue Work
Soft Tissue Prep
30-60 seconds per targeted muscle group, no more than 5/10 discomfort level
Targeted Muscular Stretching, or PNF Techniques
Hip Flexors, Quads, Groin, Calves, etc.
Lats, Teres Major, Pec Major and Minor, Thoracic Spine, etc.
Strength Work to Opposite Side of Joint
Glutes, Deep Hip Rotators, Core, etc.
Scapular Muscles, Rotator Cuff, Core, etc.
Active Flexibility in New Range of Motion and Eccentrics
Elastic band kick drills, needle kicks, PNF techniques
Elastic band openers, shoulder circles to mat laying on stomach, PNF techniques
Eccentric pull up lowers or EZ Mover Sliders
Gymnastics skill technique drills to use the new range of motion
Beam, Parallel Bar, High Bar Technique Drills Involving Splits
Beam, Parallel Bar, High Bar Technique Drills for Handstands of Behind the back motions (male gymnasts)
When this circuit approach is done with an idea of consistency over intensity, followed by proper gymnastics technique or strength programming, I think it has a substantial effect on long-lasting
flexibility changes in a gymnast. I often give these circuits for shoulder or hip flexibility assigned as homework before practice or at home. This approach is especially useful for gymnasts who are not as fortunate to be naturally mobile.
This theory is also more in line with the motor control research I have read and interpreted related to changing human movement. 95 – 97 In theory, it incorporates not only neural encoding but also motor skill acquisition and deliberate practice. By using a variety of drills that include the basic movements (hip extension, shoulder flexion with rotation, etc.) we can attempt to make more progress over time.
Lastly and most importantly, this complex approach tends to create much more engagement from gymnasts, as the longer static holding of flexibility can be very prolonged and monotonous. I feel this approach not only makes more sense from a gymnastics technique point of view, but also incorporates a lot of current scientific research on flexibility, soft tissue work, and human movement.
This will be the format I use for the joint sections below, but you can download examples of these circuits for the hip and shoulder specifically here,
Shoulder Flexibility
Screening
Seated Overhead Screen with Stick – Sitting at the wall with the lower back flat and head against the wall, the gymnast raises the bar overhead with the arms shoulder-width apart and palms down. The goal is to make hand contact with the wall. This can be repeated with the hands in an under grip to bias the muscular soft tissue of lats/teres major, can be repeated with the hands on top of each other to mimic beam for female gymnasts, and can be repeated in eagle grip for those gymnasts who perform these skills.


Soft Tissue Prep
Foam Rolling Underarm x60s
Lat Stick Stretch x60s
Thoracic Extensions Over Roller x10

Thoracic Spine Windmills x10
Active Flexibility / Eccentrics
Wall Angels Back/Seated/Stomach x10
Slider Fall Outs x10
Tucked Wall Handstands
Screening
Hip Flexibility
Right and Left Leg Split on Line
Straddle Split on Line
Soft Tissue Prep
Foam Rolling Inner Thigh x60s
True Hip Flexor Stretch x60s
Single Leg Hip Lift with Knee Hug x10
Gymnastics Specific Drills
Stall Bar Kicks x10 each
Tumble Trak Jumps x10 each (found in complex video below)
Sample Circuit
Hamstring/Pike Flexibility
Ankle Flexibility
Screening
½ kneeling lunge test at wall for Dorsiflexion (wow this video is old!)
Foam Rolling Calf Muscles
Specific Stretches
Ankle Rockers At Wall x10 reps with 10s hold at end
Goblet Squats
Jumping and Landing Drills
Wrist Flexibility
Screening
Hands and Knees Wall Rocking (for straight elbow movements) –
Soft Tissue Prep
Rolling to Inside Forearms x60s
Forearm Rock Backs x10
Bear Crawling x10 steps
Gymnastics Specific Drills
Tucked Wall Handstands x30s
Sample Circuit (again, wow old video!)
Points for Knee/Elbow Hyper Extension and Ankle Toe Point Safety
It’s very important to remember that certain joints are not inherently built for lots of flexibility. In particular, the knee and elbow joints can be areas that if overly stretched, can become problematic. As noted at the start of this article, gymnasts are typically our hyper in their joint capsules. This is associated with hyperextended knees and hyperextended elbows. If these joints are subject to ongoing stretching past their normal end ranges of motion, it can significantly increase the risk of injury.
Out of all the things I have seen in flexibility methods for gymnastics, the one that drives me the most insane is pushing knees into extension during splits or pikes. Although it’s not as common as the hip and shoulder post, I still have seen it quite a few times when in gyms. It blows my mind that people actually would push on knees for “better lines” at the cost of potentially increasing laxity in their knee and increasing the chance of a gymnast blowing ACL out during landings.
Jumping and landing athletes are already at a huge risk for ACL tears, not to mention the even higher risk for young developing female athletes. When someone pushes a knee into extension, we strain the posterior knee joint, other passive stabilizers of the knee, and tension the ACL. Given that gymnasts already straighten their knees and tend to show very knee dominant landings (versus proper hip dominant squat deceleration landings), we really don’t want to putting them more at risk for landing lock legged and having something going seriously wrong.
The ACL tear and knee injury rates in gymnastics are already high enough. It only takes one bad landing for the gymnast to suffer a major and possibly career ending injury. I strongly suggest people who may be unknowingly pushing knees down more in oversplits, or feet elevated pike stretches stop and think about why they chose to certain stretching interventions. Similar to that point, I would also be very careful about how much pressure the front knee of oversplits is taking, and if you use them try to have the gymnast move their front leg up on the mat more. We don’t want just the heel elevated with a long lever arm creating lots of posterior knee joint and ligamentous strain.
Those looking for more research related to ACL tear mechanisms can start by following this link here
- Smith et al. Risk Factors for Anterior Cruciate Ligament Injury. A Review of the Literature — Part 1: Neuromuscular and Anatomic Risk.Sports Health. 2012 Jan; 4(1): 69–78
- Smith et al. Risk Factors for Anterior Cruciate Ligament Injury A Review of the Literature—Part 2: Hormonal, Genetic, Cognitive Function, Previous Injury, and Extrinsic Risk Factors. Sports Health. 2012 Mar; 4(2): 155–161.
- Noyes FR1, Barber Westin SD. Anterior cruciate ligament injury prevention training in female athletes: a systematic review of injury reduction and results of athletic performanceSports Health. 2012 Jan;4(1):36-46.
Instead of just jumping to pushing down the knees of gymnast to get better lines or fix bent knees, I strongly suggest that people take time to figure out why the gymnast has bent knees to start with. There are many reasons, and I put together this video highlighting how to look for some of the most common ones.
Ankles are one of the most frequently injured body parts in gymnastics with a variety of injuries from getting crunched on short landings, chronic impingement, sprains, stress fractures, and more. A “rolled ankle” or inversion sprain is definitely among the most common for gymnasts. Not only do they happen quite a bit as a first time injury for a gymnast, they seem to keep popping up as re-occuring injuries for many gymnasts leading to cumulative issues down the road.
I’ve seen hundreds of them and had plenty myself during my years of gymnastics. Although I know having a fantastic toe point is something all gymnasts and coaches strive for, I personally feel that gymnasts with wobbly ankles or have a history of inversion ankle sprains shouldn’t be getting this cranked on. Here’s 3 thoughts about why.
A rolled ankle happens when the gymnast catches their foot into a “down and in” position (plantar flexion with inversion) leading to the structures on the outside portion of the foot being damaged. This often happens when the gymnast is working one legged leaps or jumps, takes off for a skill off balance, or lands with their weight more onto one leg.
Part of the reason it is so common in gymnastics is because the gymnast has to move from an extreme toe point position to a toes up landing position within an extremely small time window. If the gymnast doesn’t do it fast enough or lands awkwardly it can be problematic.
The “down” portion or plantar flexion is what makes up a toe point. Most gymnasts in general (and especially people with chronic ankle sprains) tend to hang out in this position at rest. So think about this for a second. Does it make sense to take a gymnast who go their injury in the first place by rolling her ankle “down and in” and stretch the “down” portion more?
In my mind, definitely not. Gymnasts are already notorious for having really tight calves because of how much time they spend in a toe point along with doing so much jumping and landing. Not to mention their flat feet may cause those same outside ankle structures that may be inflammed/damaged to get re-irritated when impinged upon.
If the gymnast is already hanging out in a “down and in” position, they are predisposing themselves to continuously catch their over and over, leading to the re-occuring injury part mentioned above. Cranking on their ankles to get more toe point may help to make skills look better, but may be increasing their subsequent injury risk.
Remember the biggest risk factor for an injury is a previous injury, and a lot of it has to do with what got the gymnast there in the first place. Considering what type of ankle work you are doing with a gymnast who has an injury history like this is important for coaches to think about.
This is closely related to the one above, but many of the “wobbly ankles” come about because the gymnast has lots of laxity overall. This means not only for the ankle joint, but also the rest of leg chain all the way up to the hip and lower back. Some of the gymnasts could be born more lax and likely have been successful in gymnastics because of it. Gymnastics training itself may create a position where a gymnast acquired more hypermobility with jumping/lading forces but also the large emphasis on mobility.
If a gymnast is already very mobile and lax, pushing further on the ankle joint my only be making it worse. Chances are the toe points stretch is further lengthening tendons, ligaments, and the ankle joint capsule. The gymnast is depending on those static stability structures because they probably have issues related to their muscles and nervous system not being able to assist with dynamic stability. Take this gymnast for example, who has super wobbly ankles and does a lot of pre-hab for in an effort to minimize her risk. Her ankles are very lax and she also tends to hang out in the “down and in” position that may predispose it to roll.
I would suggest that these very mobile of gymnasts need more work learning to control the motion they have both with basic movements and with complex movements that involve higher forces and fast reaction times. Teaching gymnastics specific stability and whole chain coordination through single leg jumping, hopping, dynamic balance drills, and so on is usually the more beneficial route. It can help to lower their injury risk for another ankle sprain, but it also can help their performance by increasing single leg and double leg landings/jumps etc.
A huge issue related to local ankle problems and also up the chain issues in gymnasts is the large imbalance that develops between the “toes down” motion (plantar flexion) and “Toes up” motion (dorsiflexion). Missing ankle dorsiflexion is a huge problem because it creates local ankle issues for injury but also causes a huge ripple effect up the leg chain as other joints and structures have to compensate
A huge area that this problem impacts is proper squatting, landing, and force distribution abilities during gymnastics One of the biggest things I find in gymnasts is that most of their overhead deep squat performance was pretty rough all around.
In short, stretching the toe point more may be exaggerating this imbalance, leading to issues both in their injury risk for inversion sprains as noted above but also other ankle injuries. It also may impact their ability to control landings and tumble leading to decreased performance.
There is typically much less seen where gymnasts elbows are being stretched into hyper extension, but that also should be avoided. Gymnasts should focus on maximizing wrist and shoulder flexibility, as well as doing lots of physical preparation work to strengthen the elbows.
Conclusion
So I know this has been an absolute beast of an article. If you took the time to read through everything, a major kudos to you. Even if you jumped around for bits and pieces, I hope you found them helpful. Remember, you can download the entire chapter on flexibility, the 10-minute flexibility guides, or the pre-hab guide here.
The Gymnastics
Flexibility Guide
- Cutting edge soft tissue, strength, and active flexibility techniques for splits, handstands, and shapes
- Practical traditional stretching methods combined with latest scientific research
- Techniques for increasing flexibility, and making changes transfer to gymnastics skills
We take our privacy seriously and will never share your information. Click here to read our full privacy policy.
Download My New Free
10 Minute Gymnastics Flexibility Circuits
- 4 full hip and shoulder circuits in PDF
- Front splits, straddle splits, handstands and pommel horse/parallel bar flexibility
- Downloadable checklists to use at practice
- Exercise videos for every drill included
Download SHIFT's Free Gymnastics Pre-Hab Guide
Daily soft tissue and activation exercises
Specific 2x/week Circuits for Male and Female Gymnasts
Descriptions, Exercise Videos, and Downloadable Checklists
Please share with your community, and I hope you find it helpful!
– Dave
Dr. Dave Tilley DPT, SCS, CSCS
CEO/Founder of SHIFT Movement Science
*Medical Note – Also, remember that this blog post is for educational purposes only and does not represent medical advice. I am not responsible or liable for any negative consequences that come from applying the ideas below. Please consult with medical providers for proper understanding and implementation of this information.
References
- Andrews, J., Reinold, M., Wilk, K. The Athlete’s Shoulder. Second Edition, 2009.
- Wilk KE, Arrigo CA, Andrews JR. Current concepts: The stabilizing structures of the glenohumeral joint. J Orthop Sports Phys Ther 25(6):36479, 1997.
- Wilk KE, Andrews JR, Arrigo CA. The physical examination of the glenohumeral joint: Emphasis on the stabilizing structures. J Orthop Sports Phys Ther 25:3809, 1997.
- Cordasco FA. Understanding multidirectional instability of the shoulder. J Athl Training 35(3):278285, 2000.
- Ehmke, R. S. (2006). Kinetic Anatomy. (2 ed., pp. 3556). Champagne, IL: Human Kinetics.
- Rainman, Thornburg. Clinical Examination and Physical Assessment of Hip Related Joint pain In Athletes. ISJPT 9(6) 2014.
- Alistair MM, Saran MR. Micro instability of the hip-it does exist etiology, diagnosis and treatment. Journal of Hip Preservation Surgery Vol. 0, No. 0, pp. 1-13.
- Draovitch P, Edelstein J, Kelly BT. The Layer Concept, Determining the Pain Generators, Pathology, and How Structure Determines Treatment. Cur Rev Musculoskelet Med. 2012 Mar;5(1):18. doi: 10.1007/s1217801191058.
- Weber AE, Bedi A, Tibor LM, Zaltz I, Larson CM. The Hyper Flexible Hip: Managing Hip Pain in the Dancer and Gymnast. Sports Health. 2015 Jul;7(4):34658.
- Shu B., Safran MR. Hip Instability: Anatomic and Clinical Considerations of Traumatic and Atraumatic Instability. Clin Sports Med 30 (2011) 349-367.
- Huang R, Diaz C, Parvizi J. Acetabular Labral Tears: Focused Review of Anatomy, Diagnosis, and Current Management . Phys Sportsmed. 2012 May;40(2):8793. doi: 10.3810/psm.2012.05.1968.
- Meyers CA., et al. Role of the Acetabular Labrum and the Iliofemoral Ligament in Hip Stability: An In Vitro Biplane Fluoroscopy Study. Am J Sports Med 2011 39: 85S.
- Wilk KE, Macrina LC, Reinold MM. Nonoperative rehabilitation for traumatic and atraumatic glenohumeral instability. North Am J Sports Phys Ther 1(1):1631, 2006.
- Enseki et al., Nonarthritic Hip Joint Pain: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health from Orthopaedic Section of the American Physical Therapy Association. JOSPT November 2014.
- Manske R., et al. Current Concepts In Shoulder Examination of The Overhead Athlete. IJSPT Oct 2013; 8(5): 554 – 578.
- Andrews, J., Reinold, M., Wilk, K. Current Concepts in the Evaluation and Treatment of the Shoulder in Overhead Throwing Athletes Part 2: InjuryPrevention and Treatment. Sports Health: A Multidisciplinary Approach 2(2) 2010.
- Nho, et al. Hip Arhtroscopy and Hip Joint Preservation Surgery. Elsevier. 2016.
- Weppler CH, Magnusson SP. Increasing muscle extensibility: a matter of increasing length or modifying sensation? Phys Ther. 2010;90:438 – 449.
- Ben M., Harvey LA. Regular Stretch does not increase muscle extensibility: a randomized control trial. Scand J Med SCi Sports, 2010: 136 – 144.
- Konrad A, Tip M. Increased range of motion after static stretching is not due to changes in muscle and tendon structures. Clin Biomech (Bristol, Avon). 2014 Jun;29(6):636-42. doi: 10.1016/j. clinbiomech.2014.04.013. Epub 2014 May 10.
- Nakamura M., et al. Acute Effects of Stretching on Passive Properties of Human Gastrocnemius Muscle-Tendon Unit: Analysis of Differences Between Hold-Relax and Static Stretching. Journ Sport Rehab, 2015, 24, 286 – 292
- Nelson RT, Bandy WD. Eccentric training and static stretching improve hamstring flexibility of high school males. J Athl Train 2004;39:254-8
- Cipriani DJ, Terry ME, Haines M, et al. Effect of Stretch Frequency and Sex on the Rate and Gain and Rate of Loss in Muscle Flexibility During a Hamstring Stretching Program: A Randomized Single-Blind Longitudinal Study. Journal of Strength and Conditioning Research, 2012; 26(8) 2119 – 2129.
- Harvey L, Herbert R, Crosbie J. Does stretching induce lasting increases in joint ROM? A systematic review. Physiother Res Int 2002;7:1-13.
- Thomas E., et al. The Relationship Between Stretching Typology and Stretching Duration: The Effects on Range of Motion. Int J Sports Med. 2018: 39; 39: 243 – 254
- Herbert RD, Gabriel M. Effects of stretching before and after exercising on muscle soreness and risk of injury: a systematic review. BMJ 2002;325:468.
- Zollner AM., et al. Stretching Skeletal Muscle: Chronic Muscle Lengthening through Sacrocmeregenesis. PLOS, 2012, 7(10): 1-10
- Kubo K., Kanehisa H., Fukunaga, T. Effect of stretching training on the viscoelastic properties of human tendon stiffness in vivo. J Appl Physiol, 2002, 92: 565 – 601
- Konrad A, Gad M, Tilp M1. Effect of PNF stretching training on the properties of human muscle and tendon structures. Scand J Med Sci Sports. 2015 Jun;25(3):346-55. doi: 10.1111/sms.12228. Epub 2014 Apr 10.
- Shibata KR, Mastuda S, Safran MR. Is there a distinct pattern to the acetabular labrum andarticular cartilage damage in the non-dysplastic hip with instability? Knee Surg Sports Traumatol Arthrosc. 2016.
- Riboh JC, et al. Atraumatic Hip Instability in Patients with Joint Hypermobility.Operative Techniques in Sports Medicine. 2015; 23: 203-212
- Escamilla RF, Hooks TR, Wilk KE. Optimal Management of Shoulder Impingement Syndrome. Open Access Journal of Sports Medicine 2014:5 13-24
- Edwards SL, Bell JE, Bigliani LU. Subacromial Impingement. In Wilk KE, Reinold MM, Andrews JR., The Athlete’s Shoulder: 2nd Edition. 2009. Philadelphia: Churchill Livingston. 115-122
- Reinold MM, Curtis AS. Microinstability of the Shoulder in the Overhead Athlete. IJSPT. 2013l 8(5) 601 – 616
- Hart E., et al. The Young Injured Gymnast: A Literature Review and Discussion. Curr Sports Med Rep. 2018 Nov; 17(11)
- Macdonald GZ, et al. Foam rolling as a recovery tool after an intense bout of physical activity. Med Sci Sports Exerc. 2014 Jan; 46(1): 131-14
- Herbert RD1, de Noronha M. Stretching to prevent or reduce muscle soreness after exercise. Cochrane Database Syst Rev. 2007 Oct 17;(4):CD004577.
- Sands WA, Flexibility. In Cardinale M, Newton R, Nosaka K,Strength and Conditioning: Biological Principles and Practical Applications. 2011. John Wiley & Sons: Oxford. 389 – 398
- Sands WA, McNeal J. Mobility Development and flexibility in youths. In Llyod RS, Oliver JL, Strength and Conditioning for Young Athletes: Science and Application. 2014. Routledge: New York. 132 – 146
- Sands WA, McNeal J. Flexibility: developing effective movement. In Jeffreys I., Moody J. Strength and Conditioning for Sports Performance. 2016. Routledge: New York. 387 – 403
- Beardsley C, Skarabot J. Effects of self – myofascial release: A systematic review. J Bodyw Mov Ther. 2015. Oct; 19(4): 747 – 758.
- Schleip, R. Fascial Plasticity: A New Neurobiological Explanation: Part 1. Journal of Bodywork and Movement Therapies, 2004.
- Kalichman L1, Ben David C2. Effect of self-myofascial release on myofascial pain, muscle flexibility, and strength: A narrative review. J Bodyw Mov Ther. 2017 Apr;21(2):446-451. doi: 10.1016/j.jbmt.2016.11.006. Epub 2016 Nov 14
- Bialosky, et al. The Mechanisms of Manual Therapy in the Treatment of Musculoskeletal Pain: A Comprehensive Model. Man Therapy 2009. Oct 4 (15).
- Chaundry H, et al. Three-Dimensional Mathematical Model for Deformation of Human Fasciae in Manual Therapy. J Am Osteopath Association. 2008;108:379390.
- Ogura Y, Miyahara Y, Naito H, Katamoto S, Aoki J. Duration of static stretching influences muscle force production in hamstring muscles. Journal of Strength and Conditioning Research. 2007. 21, 788-792
- Yamaguchi T1, Ishii K, Yamanaka M, Yasuda K. Acute effect of static stretching on power output during concentric dynamic constant external resistance leg extension.J Strength Cond Res. 2006 Nov;20(4):804-10.
- Opplert J, Babault N. Acute Effects of Dynamic Stretching on Muscle Flexibility and Performance: An Analysis of the Current Literature. Sports Med. 2018 Feb;48(2):299-325. doi: 10.1007/s40279-017-0797-9.
- Healey KC, et al. The effects of myofascial release with foam rolling on performance. J Strength Cond Res. 2014 Jan;28(1):61-8. doi: 10.1519/JSC.0b013e3182956569
- Peacock CA, et al. An Acute Bout of Self-Myofascial Release in the Form of Foam Rolling Improves Performance Testing. Int J Exerc Sci. 2014 Jul 1;7(3):202-211. eCollection 2014







