Knee Injuries in Gymnastics – A Complete Guide

In gymnasts, the knee joint has the highest rate of “severe” injuries. Unfortunately, this refers to injuries tending to cause the most tissue damage and pain when they occur. Many knee injuries also tend to create the most missed time from training and competition. Lastly, as long-term studies have suggested, there is a concerning trend for athletes who suffer injuries like ACL tears having long-term issues related to knee injuries they experienced when younger.
Due to these concerning concepts in research studies, and the unfortunate reality that 1000s of gymnasts still struggle with knee injuries each competitive season, we must take more dedicated actions to help. In an ongoing effort to provide high-quality, science-based education to the gymnastics community, I have started this “mega-blog” series. My hope is that by laying out the current science as I understand it, and by describing it in a way that is accessible to everyone in the gymnastics community, we can all work together to make a positive impact on reducing the rates of knee injuries in gymnastics.
As a former collegiate gymnast, I understand all too well how brutal these injuries can be. I struggled with various knee injuries during my career and watched many of my teammates go through surgeries for ACL tears, meniscus tears, fractures, and more. Now as a Sports Physical Therapist, Strength Coach, Gymnastics Coach, and Researcher, I have (unfortunately) had to help thousands of gymnasts with various knee injuries.
After this short introduction, I will start by outlining how common knee injuries are in gymnastics. I will then review some of the biggest factors that might be most important to understand as to why these knee injuries occur. Following this, I will break down the basic anatomy of the knee joint and the most common knee injuries we see frequently in gymnasts. Then, I will walk people through the 4 main phases of injury rehabilitation, share the exact exercises/approaches I use with gymnasts, and talk about returning to sports safely. To conclude things, I will discuss some ways that we can work together to reduce the risk of knee injuries in gymnastics and offer help for people who may be struggling with ongoing pain.
Table of Contents
In-Depth Courses for Gymnastics Coaches and Gymnastics Medical Providers
Before going down the rabbit hole, I know that many people want a “step by step” instruction guide for fixing gymnastics knee injuries.
If you are a gymnastics coach, I have 40+ of webinars, handouts, and discussion boards inside our online gymnastics education group The Hero Lab. We cover everything from flexibility, to strength, to culture, and more while getting access to monthly “Office Hour” live Q&A’s.
For Gymnastics Medical Providers, I have an 8.5 hour PT/AT CEU approved course where I will teach you exactly how I treat gymnasts for hip, knee, and ankle injuries called Evidence-Based Evaluation and Treatment of Lower Extremity Injuries in Gymnasts. You can check them below out if that fits your fancy.
![]()


If you prefer to listen to this in podcast form or watch it in video form, you can check those out here!


![]()
How Common Are Knee? Injuries in Gymnastics?
To first understand how common knee injuries are in gymnastics, let’s review some epidemiological studies. These are studies that look at the rates and prevalence of certain injuries within different areas of gymnastics.
- O’Kane 2011, 96 Club level gymnasts Level 4-10
- 14% of injuries were to the knee
- Westerman 2015, a 10-year study of 121 gymnasts in the NCAA
- 1.21 knee injuries per 1000 exposures male gymnasts, 2.10 knee injuries per 1000 per exposures male injuries
- 26 major knee injuries requring surgery (ACL tears, meniscus tears, etc)
- Kerr 2015 in NCAA Gymnasts, 11 programs with 418 injuries over 5 years
- 50% of injuries were in the lower extremity, 10.3 were knee
- Knee had the highest rate of “severe” injuries requiring surgery
- Floor was responsible for the most knee injuries, due to repetitive impact
- Kolt 1999 of 64 elite and sub elite gymnasts over 18 months
- 13.5% of injuries were to the knee
- Hudash 1993 of 26 NCAA Gymnasts over 4 year period 1983-1987
- Most common inuuries were patellofemoral pain (22.7%), synovitis (18.1%), tendonitis (13.6%), and sprains (13.6%)
- Salun et al 2015, 21 year study of 3681 injuries from elite/intermediate/novice level
- 17.0% of all injuries, totally 627 injuries
Why Are Knee Injuries So Common in Gymnastics?
High Impact Landing Forces
Looking at the studies above, almost all of the knee injuries recorded came from various forms of impact. In gymnastics, there are different forms of impact. One is the “technique” based impact that comes with tumbling, punching, or bounding. This involves a more stiff, rigid, body posture that allows the gymnast to utilize the equipment (springs in spring floor or board, balance beam, etc) to create bounce and perform skills.
Sometimes, the repetitive nature of bounding and impact on these events can cause issues like patellar tendonitis or growth plate injuries like Osgood Schlatteres to surface. Also due to the knees being relatively “stiff” during punching, accidents can happen with locked-legged landings that may create ligament sprains or bone bruises. Some of these are unavoidable, but working on air awareness, technique, leg/core strength, and workload management have been suggested to help.
The other type of impact comes from landing skills or dismounts. This type of impact is a huge contributor to high rates. of overuse and sudden traumatic knee injuries in gymnastics. Landing should involve using a traditional squat-based movement to help absorb extremely high forces (more on that later). The forces of sprinting are also common in gymnastics, but these are not nearly as high as landings.
The forces of gymnastics tumbling and landings are massive, ranging from 15-18x bodyweight (more in this textbook here and here). In fact, the highest recorded forces that we know of were measured at the ankle joint during the take-off of a double back on floor and reached up to 23x bodyweight (more in this textbook here and here).
Keep in mind, this data mostly comes from controlled settings and definitely does not reflect all of the “real-life” situations of gymnasts landing short, more on one leg, or awkwardly. Many of the highest stress situations on the knee likely haven’t been fully studied. This is just a tough reality that we have to face in gymnastics, but if we face it head-on we can look at ways to help like strength and conditioning.
High Impact Repetitions
Along with high-impact forces, another reality of gymnastics is that it is HARD. By hard, I mean the skills themselves are extremely challenging to learn, master, and compete. Even the most basic skills take years to get a handle on. Due to how hard the skills are, it often takes thousands of repetitions to make progress. With the proper dosage, drills, and monitoring, these impact forces can actually be beneficial and help athletes adapt.
Unfortunately, for many in the sport, this type of approach might be lacking. These repetitions can come at a huge cost when not properly planned for or dosed in training. Young gymnasts may end up taking thousands of high-impact repetitions per month without proper strength, skill technique, or recovery. This can create a situation where various tissues in the knee joint and muscles supporting it get overused and start to develop pain or injury. Or, it could create a situation where the athlete is exposed to really high impact forces before they are mentally or physically ready, creating an acute injury. With this in mind, we must look to education, the use of matting to buffer forces, and strength & conditioning to help combat risk.
Gymnasts Being Young & Pre Puberty
Another tough pill to swallow – the majority of athletes training in gymnastics are children. Despite ages trending upward for the world and Olympic teams, the vast majority of people competing in gymnastics are under the age of 16. They are young kids, who have yet to fully develop physically or mentally. This means, according to great research and textbooks, they are nowhere near their peak strength, power, or cardiovascular capacity.

Not to mention, their growth plates are wide open and very vulnerable to injury. If gymnasts are not developed enough or lack the physical preparation to protect their knee joints and open growth plates, injuries like Osgood Schlatters might stack up fast. It’s crucial that young gymnasts have the core, hip, leg, and knee strength to help buffer these high forces going through their knee joints and growth plates that are not fully formed yet.
Gymnastics is a very unique sport where very young kids ages 8-12 are asked to perform very high force skills, in high amounts, and are training 20+ hours per week in some situations. In some areas of the sport, particularly those trying to get on the pre-elite/elite or NCAA track, it can create a difficult time period where pre-pubertal athletes are training high force skills, in high repetition, well before their bodies are physically or mentally capable of handling it. This is where expert coaching, training plans, and pacing comes must be a priority.
Lack of Science-Based Strength & Conditioning Methods
This is something that applies to all gymnastics injuries but in particular lower-body injuries of the knee. As mentioned, the knee joint has the higest rate of “severe” injuries in gymnastics. Looking at the literature on ACL tears, tendinopathy issues, and more, there are two huge modifiable factors – strength & conditioning and teaching proper landing patterns – that are still not being utilized to their fullest potential in gymnastics.
Based on great literature (more here, here, and here), it is clear that a properly done, properly coached, and properly progressed strength and conditioning program is beneficial for performance and reducing the risk of injuries. This includes a combination of both external weight lifting and bodyweight strength work. Taking this one layer further, a lower body strength program can be insanely beneficial in a jumping/impact-based sport like gymnastics.

Despite the abundance of evidence, there is still a huge percentage of gymnastics professionals who feel that gymnasts should not be lifting weights. They fear myths and misunderstandings about weight training, believing that it will make gymnasts “bulky”, less flexible, and cause injuries. However, a closer look at the literature show this to be largely false, given the program is properly implemented and coached with an aim of improving explosive power. Even more so, it is clear that weight training is not only not dangerous for kids, but likely helpful in reducing injury risk.
As a result of this cultural barrier, many gymnasts do not get the adequate leg strength and capacity needed to handle the high-impact forces going through their knee joints. Not to mention, they are putting a huge bottleneck on their potential to train and compete for high-level skills. Gymnastics is a sport based on explosive bodyweight power. The same thing that helps improve this power will also help mitigate the risk of knee injuries, overuse, and acute. For more information about this topic check out this popular blog post I wrote in 2016.
Also, if you would like to read my “Ultimate Guide to Gymnastics Strength” – you can check it out here.
Improper Landing Techniques Still Taught & Used
By far and away, one of the biggest changes that must be made in gymnastics to reduce the risk of knee injuries is a sport-wide adoption of using science-based landing mechanics. It is unclear whether this comes from a lack of education, an ‘old school’ mindset, or a desire to mimic the esthetic type landing seen in ballet or dance.
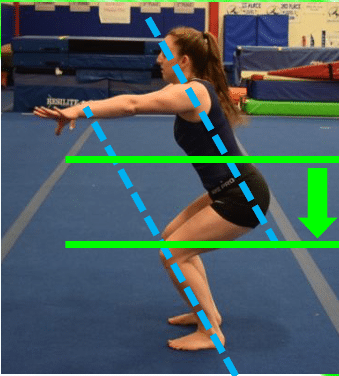
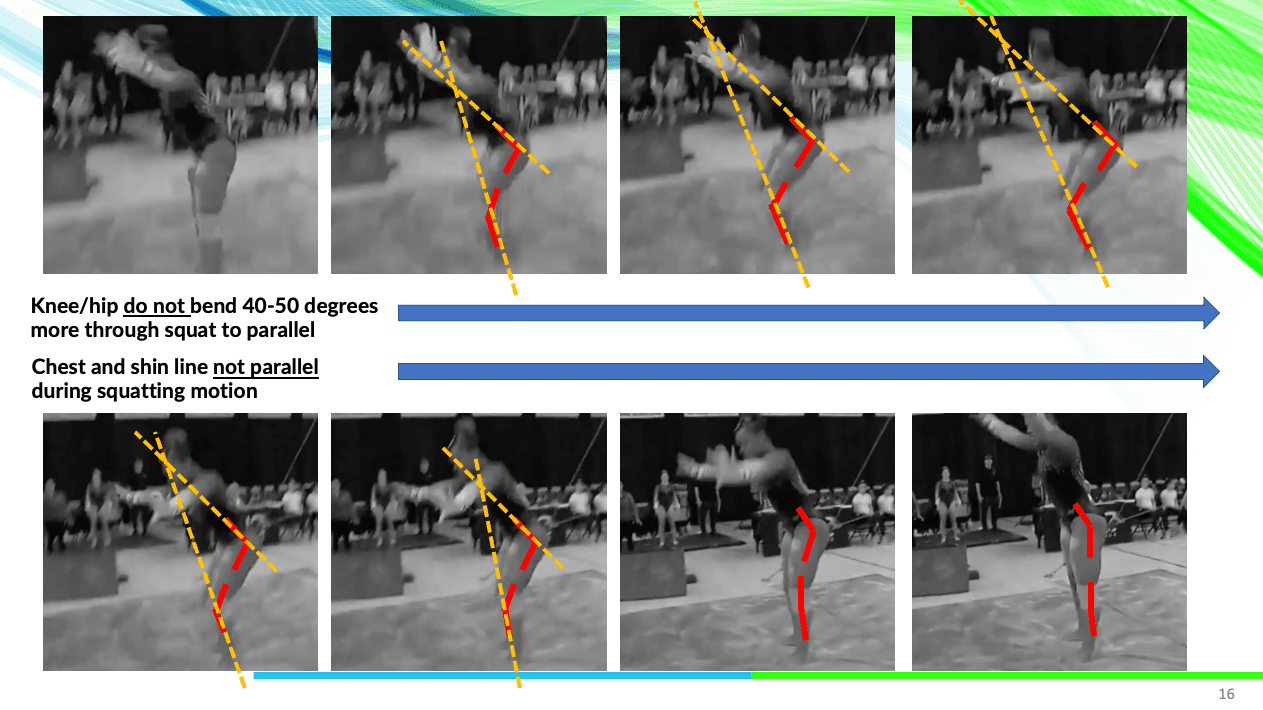
However due to this, many people in gymnastics still teach use, and judge, based on a landing position that is not supported by science to ideally help dissipate high forces. Many gymnasts still land with their feet together, torso upright, hips tucked under, and in a ‘knee’ dominant patterns that may shift more stress onto the knee and ankle joints.

This is in contrast to the suggested landing pattern, supported by enormous amounts of data in the knee injury literature, of a squat based landing that has the feet hip-width apart, knees tracking in line with the hip and feet, and the allowance of squatting to parallel depth so various musculature can be recruited to buffer forces.
Until this becomes the gold standard for teaching gymnasts how to land in practice and competition, we may continue to see high lower-body injury rates. I recently gave big presentations to the coaches and judges in the NCAA about this topic that you can check out here.
Sport Culture – Early Specialization
One of the most important, yet most challenging, issues at hand is changing gymnastics culture. The last five years have clearly shown us that there are many dark corners of a gymnastics training culture that exist in “old school”, archaic methods being used. There has been a massive amount of scientific data published around early specialization (here and here), year-round training (here and here), strength and conditioning (here and here), workloads (here and here), that have yet to make their way into mainstream gymnastics training.
Early specialization, when an athlete chooses to only participate in one sport, is one of the biggest concerns. It is common to hear gymnasts being told they will ‘miss their shot’ if they don’t only do gymnastics from a young age. While I do believe that gymnasts, particularly those with high-level goals, may need to specialize earlier than most sports, asking a 6 or 7-year-old to only train in gymnastics and not experience other sports is asking for disaster.
There is great evidence that this is concerning for increasing the risk of burnout, overuse injuries from repetitive movement patterns, and that it may negatively impact their overall athletic potential long term. The majority of the literature suggests that 14 or 15 years old is ideal for specialization. With that in mind, I think that may be unrealistic for many gymnasts, and that 10-11 might be a better target. But hearing about gymnasts specializing at 8 years old, as studies including one in the NCAA I was part of have suggested, is definitely concerning for all injuries but knee injuries in particular. This is something our sport desperately needs to talk about and change to protect young at-risk gymnasts. While there is a large range of movements in gymnastics, the repetitive impact of only doing gymnastics from a young age might be a big reason so many knee injuries occur.
Sport Culture – Year-Round Training
Year-round training is another concerning cultural phenomenon that continues to persist in gymnastics. As with early specialization, there is an abundance of research across many sports (more here , here, and here) suggesting that athletes who train more than 9 months out of the year in a single sport are at elevated risk of injury and burnout. This has been well studied in baseball, which is a sport I’m fortunate my mentors Mike Reinold and Lenny Macrina were pioneers in alongside current studies like this.
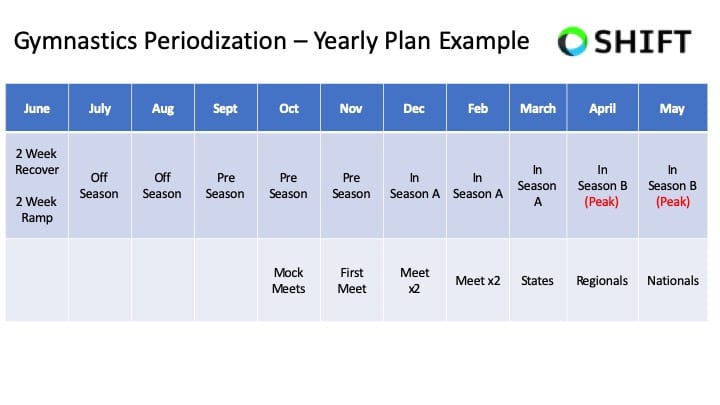
I strongly feel that creating relative off-seasons, using periodization, and utilizing cross-training are crucial for reducing knee injury risk and optimizing performance. The reality of our sport is that there has never been a time when gymnasts followed evidence-based guidelines around recovery, offseasons, and science-based work to rest ratios.
My hunch is that remodeling our year-to-year approach, shortening competitions seasons, and giving athletes a relative off-season after their hardest meet, would yield massive improvements in health and performance. I think the COVID pandemic is a further support piece of this, where many gymnasts said that after 2-3 months off, they felt the best they have ever felt mentally and physically. I don’t think it’s wise to give gymnasts extended periods of time fully off each year (3+ months for example). Hower, 4-6 calculated weeks would likely be incredible for athletes, coaches, and parents.
Lack of Science-Based Workload/Wellness Monitoring Programs
Workload, athlete monitoring, and periodization are all areas of research that have become very popular in sports around the world. It is very common to hear about sports like soccer, basketball, and baseball utilizing specific workload tools to help plan and manage training volumes in athletes.
While there has been more conversation about workload management in gymnastics, the current approach still largely depends on a coach’s perception for decisions to be made. This was recently shown in Rhythmic Gymnastics but is likely the case in other domains such as artistic, trampoline & tumbling, and more.
The truth of the matter is that while there is some data in forces on the knee, we still have a tiny fraction of what is needed to create evidence best training plans around impact and health. We have no idea what the impact forces on the knee joint are for a Tumbl Trak, vs Trampoline, vs a rod strip, vs a new spring floor, vs an old spring floor, vs a spring floor with a sting mat for take-off or an 8″ mat for landings. By not knowing these numbers, and by not having a logical progression of forces over multiple weeks, we are essentially asking coaches to fly a plane without any speedometer or gas gauge. It’s insane, and a huge reason we continue to see so many gymnasts struggle each year.
If we hope to curb the number of knee injuries in gymnastics, it is imperative that we look into better tools for external and internal workload tracking. Without knowing what the forces of different surfaces are on the foot/ankle, and how to keep a close eye on the training load gymnasts take, it’s like trying to fly a plane without any gauges or speedometers.
While this is evolving in gymnastics and is a field I’m actively doing research in (see below), the reality is we still have a long way to go. We desperately need research to be conducted on the different forces on the knee joint during tumbling, vaulting, and dismounts. We also need better systems in place to monitor how athletes are responding to gymnastics-specific training. This will help us enormously to plan, track, and keep in touch with how gymnasts are doing.

Lack of Science-Based Flexibility Methods
While this is not one of the most significant factors for knee injuries, it still does play a role in them due to how important large ranges of motion are to gymnastics.
More challenging jumps, leaps, and gymnastics skills tend to demand more lower body flexibility. Due to this, on a daily basis various flexibility exercises are performed for the quadriceps, hamstrings, and groin muscles to help gymnasts improve range of motion. While this is definitely good, and important to do, the methods in which some people use to achieve those changes might not be in line with the current literature.

While gymnastics culture is full of overly aggressive methods like very prolonged static stretching into oversplits, using ankle weights to achieve bigger jumps/leaps, and excessive pushing during splits (which is VERY dangerous when improperly done) there is literature that contradicts these as being the most optimal methods.
This study by Thomas outlines many evidence-based ways to improve range of motion safely with a ‘consistency over intensity’ mindset, while this study supports the role of eccentric strength training, and this study discusses how actual tissue changes may not be the main role for stretching improving range of motion. These studies have been available for years, but have yet to truly make their way into gymnastics culture.
When proper science-based methods are not used for stretching, it may not only stall progress but may also be a contributing factor to various knee injuries. Whether we are talking about excessive pressure on growth plates or lacking the flexibility to get into a proper squat pattern to absorb forces, applying this science correctly is essential if we wish to see progress here.
If you would like to read my “Ultimate Guide to Gymnastics Flexibility” – check out this very popular blog post here.
Gymnastics Basics/Foundational Technique Sometimes Not A Focus
On the sport-specific side of things, it has to be mentioned that technology itself is a huge factor in injury risk for gymnastics. While there is not as much scientific evidence looking at different types of gymnastics skill techniques, it’s paramount the gymnasts are taught proper basics, foundational techniques, and progressions.

This is particularly true for the knee joint, where the bounding and punching technique is crucial. Gymnasts must be put through the proper technical progressions for vaulting, tumbling, acro series, trampoline bouncing, and more to make sure they are equipped to handle the high forces of skills. If these foundations are not set from an early age, and a constant focus as the gymnast progresses in level, it might create high-risk situations. Making changes here comes down to better coaching and education systems throughout the world, to share. the optimal technique and progressions to keep gymnasts as safe as possible.
Equipment Technology Progression
Lastly, there is no denying that the sport of gymnastics has become exponentially harder in the last 10 years as equipment technology progresses. The spring floor, the vaulting table, the trampoline beds, and other advancements have helped skyrocket the level of skills being performed. The double-edged sword here is that this also increases the average force the body takes.
While the landing surfaces and matting have also increased in their ability to protect athletes’ ankles and feet, the net increase in force is still substantially higher in today’s gymnastics environment. It also creates a small ‘ripple effect’ on the younger generations, where the nature of harder skills being performed means that more time, effort, and possibly starting to learn these skills at a younger age, also occurs. Coaches must be trained on how to use different equipment for proper progressions, and we also have to financially support gyms that need better equipment to keep athletes safe.
Basic Knee Anatomy As It Relates to Injuries
I by no means am here to bore people with a dissertation in anatomy. But if we wish to make a change in the rates of knee injuries, we must first understand the anatomy that contributes to those injuries. This helps to understand the nature of common injuries and leads us down the road of helpful strategies to reduce risk.
If you want all the scientific textbooks and anatomy references to look up, check out this textbook, and some helpful research articles here, here, here, and here.
Layer 1 – Bones
Tibiofemoral Joint

There are two main bones that make up the first portion of the knee joint. The bottom of the thigh bone, known as the femur, extends down to form the top portion of the main knee joint. The top of the main shin bone, known as the tibia, extends up to form the bottom portion of this main knee joint. The meeting of these two bones makes up the joint that is is the primary reason the knee joint bends and straightens, but does allow for small bits of rotation. It is known as the tibiofemoral joint.
The bottom of the femur bone has very large, thick cartilage on the surfaces that bear weight. It serves to help disperse large impact forces that occur during weight-bearing, bending, and impact. The top of the tibia bone also has cartilage that covers it, but also large circular pieces of fibrocartilage known as the meniscus that further help disperse high impact forces. We will talk more about these below.
Patellofemoral Joint
A third bone, known as the patella, is circular and sits on the front side of the two bones mentioned above. It serves to increase the force the quad muscles can exert to straighten the knee. It also serves to assist in gliding during knee bending and also has cartilage on the backside of it that further helps spread out high compression forces. The junction of this patella with the femur is known as the patellofemoral joint.
While not directly part of the joint that bends the knee, the fibula also important to role. While it does not bear much weight, it does serve a very important role as an attachment point for certain ligaments and soft tissues. As I’ll talk about below, the LCL ligament does attach to the top of the fibular. Due to it’s involvement in some knee injuries, it’s important to note.
The Train Analogy
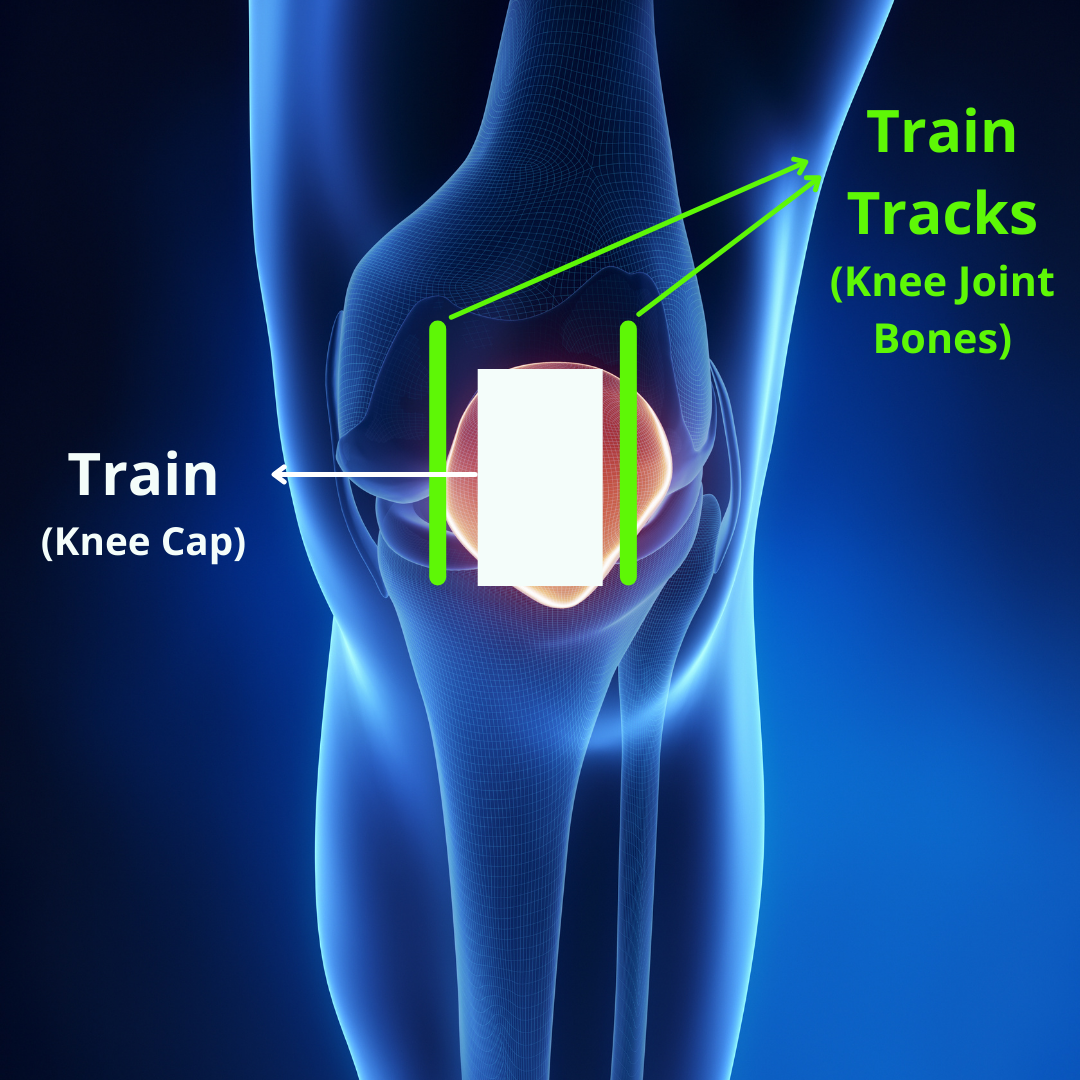
One of the most useful analogies I use with patients or when teaching, is that of a knee being much like a train gliding on a train track. The tracks are representative of the femur bone meeting with the tibia bone, creating the tracks upon which the train moves. This is formally known as the trochlear groove. The train is representative of the patella, which moves along the track during bending and straightening of the knee.
However, there are some unique features to this train/train track situation that are worth noting. First, unlike a real-life train setup, the “tracks” of the knee joint can twist or shift a bit underneath the train. Movement of the lower back and hip joint can influence the end of the femur bone’s position. Movement at the ankle joint can influence the top of the tibia bone’s position. Also, depending on whether the foot is planted on the ground during knee bending, or not planted on the ground, will change how the knee joint glides and rolls. This is why it’s crucial to evaluate and treat the lower back, hip, knee, and ankle joint together as one unit.
Second, the “train” of the knee joint does not only move straight down and up on the tracks as a train may move straight front to back in real life. The patella moves down, up, side to side, and tilts in all 4 directions during motion. This is a very important part of knee injuries, as regaining the natural multi-directional gliding motion of the knee cap is what sets the stage for returning back to high-level strength, power, and sporting movements. With these caveats in mind, this is a useful analogy to carry through in the worst of this blog post.
Layer 2 – Ligaments/Joint Capsule
The knee joint capsule is an important structure. I describe it to people as a thick Saran wrap-type balloon structure that wraps around the entire knee joint. It has within it synovial fluid, which is crucial to not only lubricate the joint for smooth gliding but also provide nutrition. It also provides some extra stability. This joint capsule can not only be the source of much fluid accumulation but also can sometimes lead to issues with limited range of motion and pain.
Ligaments on the other hand are much more specific structures. Where the joint capsule is broad and encompasses the entire knee joint, ligaments are very particular structures that span from one location to another, and resist certain motions. There are many, many ligaments and portions of the joint capsule that may be injured, so I will only cover the main ones as it relates to gymnastics.
For all ligaments, things typically follow a Grade I – Grade III scale, with Grade I being less severe and grade III being the most severe. In a grade I sprain, the ligament is stretched and irritated, but microlearning does not occur. While it can still create swelling and pain that limits sports participation, typically it only requires 4-6 weeks to see good healing.
In Grade II tears, more damage occurs as the ligament is overstretched to the point where micro-tearing occurs. This leads to much more pain, swelling, and tissue damage. Visible bruising or enlargement of the knee is seen, and most athletes have to modify their walking with crutches or a brace for a period of time. Depending on the ligament damage, surgery may be required.
The ACL and PCL for example, are within the knee joint capsule and have less direct blood flow as well as less inherent healing capacity. They are also more primary in their role to help the knee during bending or straightening. When Grade II tears occur, a surgical repair that uses a graft (quad, patellar tendon, hamstring tendon, etc) is typically opted for in athletes to reduce the risk of further injury. The MCL and LCL, on the other hand, are outside of the knee joint capsule and get much better blood flow that predisposes more healing capacity. Oftentimes, surgeons will recommend a period of rest, bracing, restriction range of motion, and rehabilitation while allowing the ligament to scar down and heal.
Unfortunately, there are times when the high forces of gymnastics landings willfully tear the ligament. These are Grade III injuries. They tend to be the hardest to deal with, as they come with notable tissue damage, pain, swelling, and interference with movement. They most often require surgery and extensive periods of rehabilitation following repair or reconstruction.
Due to the unique design and function of the knee joint, it is common to see multiple ligaments or structures damaged at the same time. For example, in what is known as the “Unhappy Triad”, the ACL, MCL, and medial meniscus are all damaged. Also, a significant bone bruise typically occurs between the outer femoral condyle and inner tibial plateau, which some studies suggest can be one of the biggest generators of pain and limited motion.
With this in mind, let’s review some of the main ligament and more passive structures of the knee.
ACL (Anterior Cruciate Ligament)
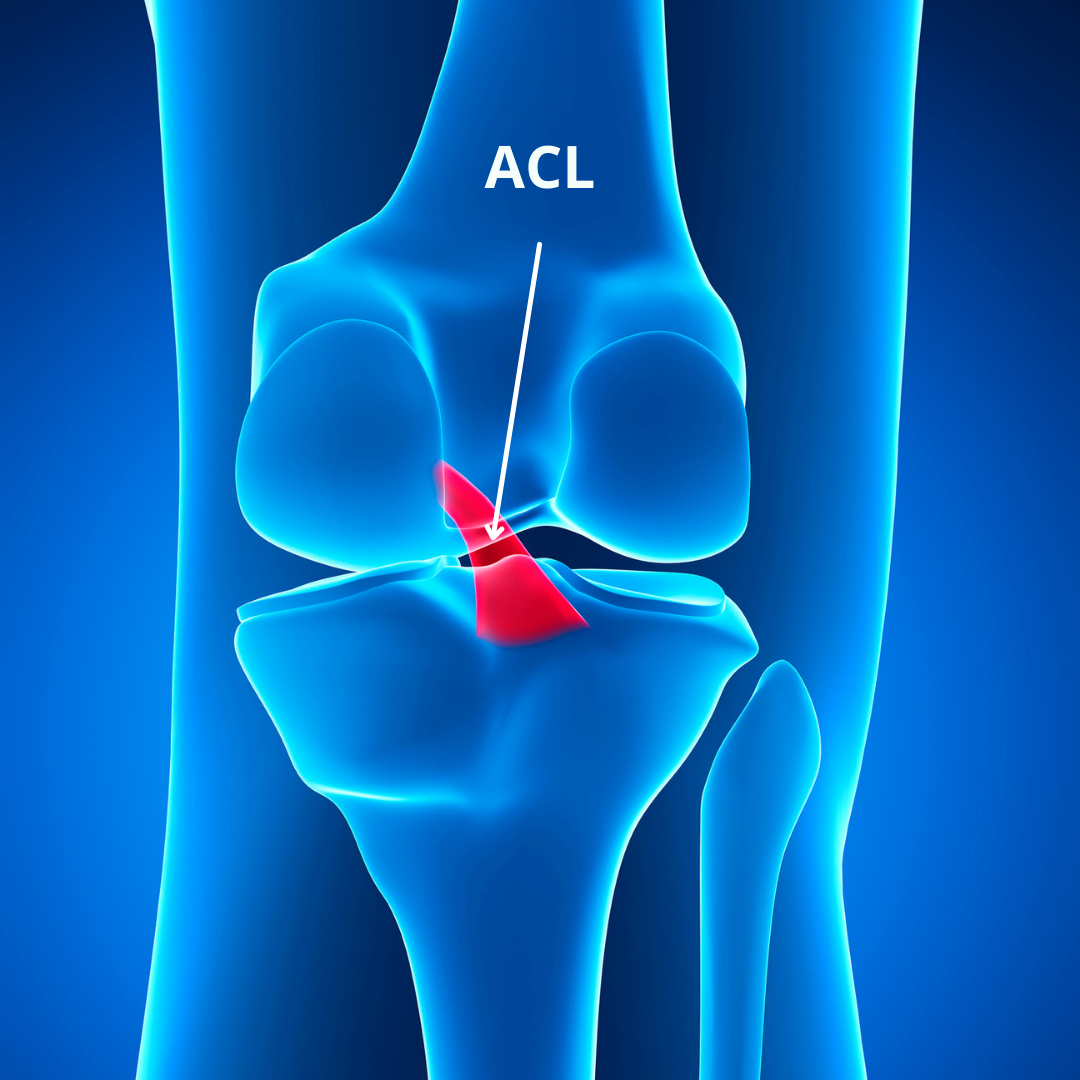
This is the most famous ligament within the knee joint, due to its high rate of injury and high possible negative impacts on an athlete’s career. This dual blended bundle ligament starts from the outer side of the femur bone, travels obliquely across the knee joint, and attaches to the front of the tibia bone between the menisci. It serves to prevent excessive forward and inward rotation of the knee joint, particularly during impact and landings. Its main mechanism of injury is rapid ‘caving’ of the knees (called dynamic valgus). It can also be injured with hyperextension of the knee that commonly occurs during landings in gymnastics.
PCL (Posterior Cruciate Ligament)

This ligament works in opposition to the movements restrained by the ACL. It starts from the inside portion of the femur, runs obliquely through the knee joint, and then inserts on the back of the tibia bone between the meniscus. It serves to prevent excessive backward and outward rotation of the knee joint. This type of injury is typically rarer but can occur during hyperextension landings that might have rapid compression load.
MCL (Medical Collateral Ligament)
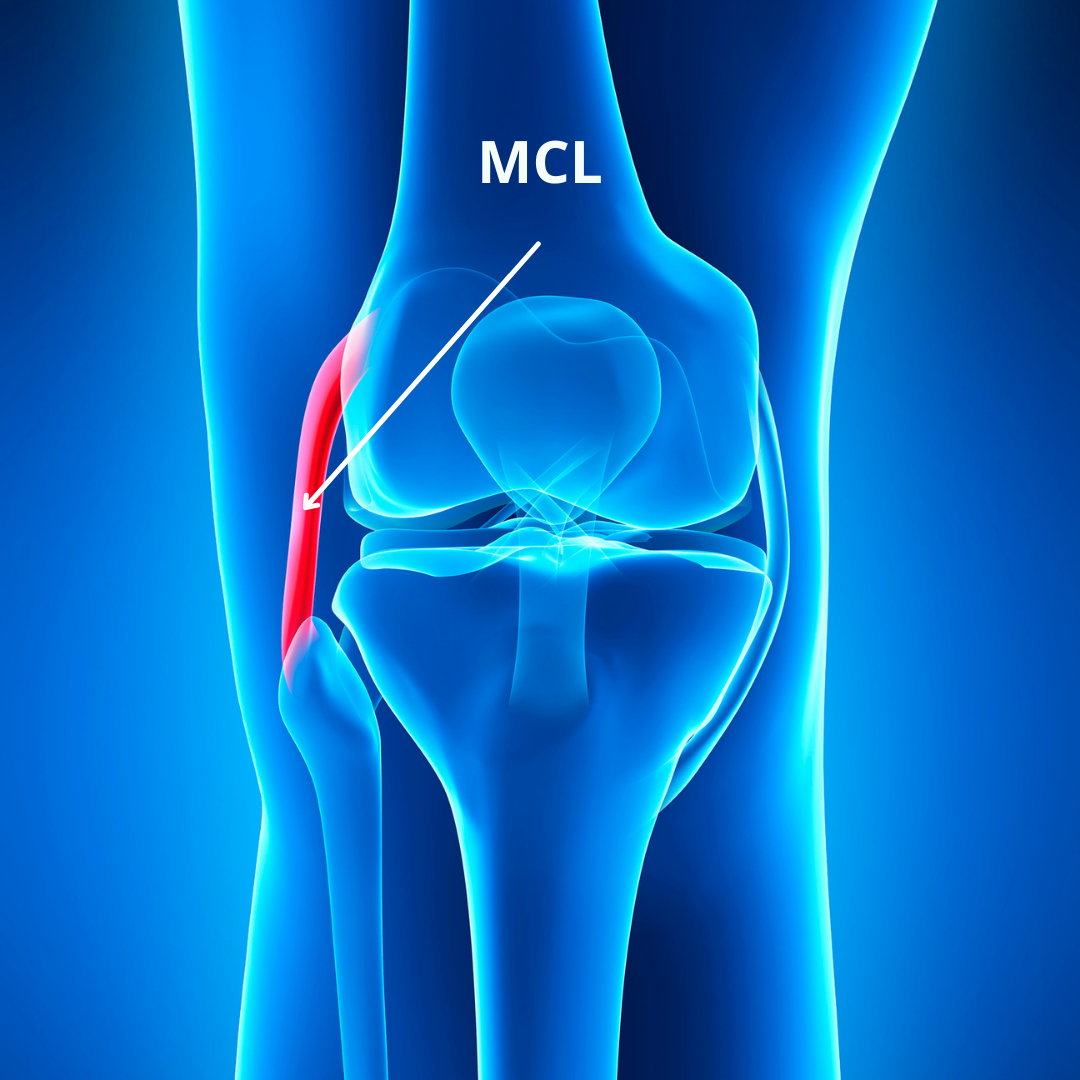
The MCL ligament starts from the inside part of the femur bone and travels downward until it attaches to the top and inside portion of the tibia bone. This ligament is commonly injured either in isolation or in conjunction with an ACL tear. This is because the MCL ligament mainly serves to prevent excessive inward ‘caving’ of the knee joint where gapping of the knee joint may occur. This is known as a ‘valgus’ force on the knee. It can also be further stressed with excessive inward rotation of the knee joint, or situations in which the knee is rapidly bent and twisted at the same time.
Due to the MCL being outside the joint capsule, there is often much more swelling, inside knee pain, and lost motion into bending when injuries occur. Athletes may or may not feel a distinct pop, depending on the severity or grade of the injury. Special tests such as pain with touching the ligaments a figure 4 position (which gaps the joint and stresses the ligament) or a valgus stress test may raise suspicion of an MCL injury. Follow-up MRIs can be performed to help gauge the severity of the injury. It’s also worth mentioning that often times athletes will have pain on the outside of the knee joint as well, due to the possibility of the outer portions of the knee joint hitting each other creating a bone bruise.
LCL (Lateral Collateral Ligament)
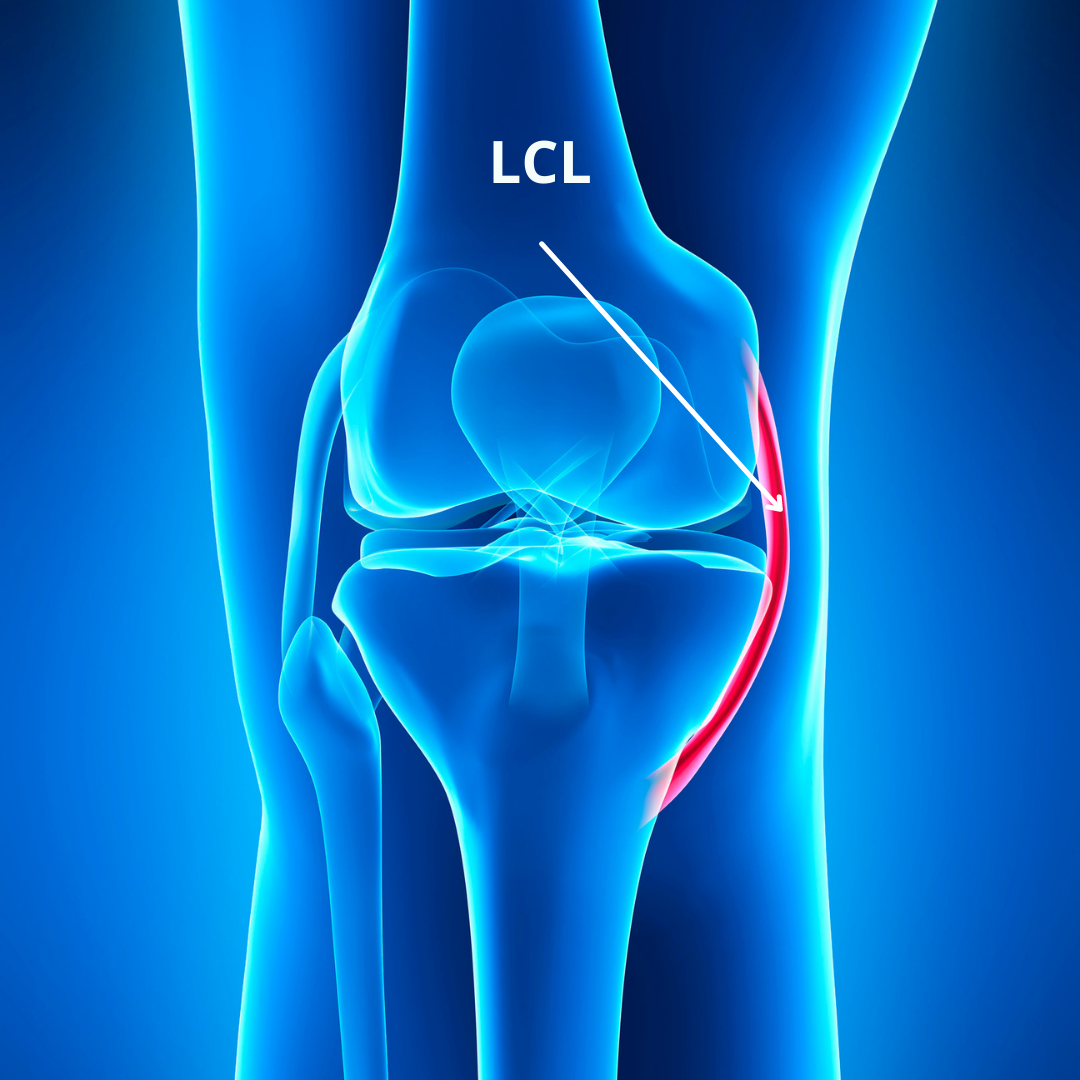
The last of the 4 main knee joint cruciate ligaments is the LCL. As the counterpart of the MCL, it starts from the outside portion of the femur and extends down to attach to the outside portion of the tibia bone. It is not as commonly injured, as extreme outward bending force is required to cause damage. This force, known as a ‘varus force’ usually only occurs in very awkward landings on a single leg. As contact from another person is not a part of gymnastics, this mechanism isn’t as common.
As in the other major ligament injuries, special tests like direct palpation of the ligament and a varus stress test can be used if an LCL injury is suspected. From there, an MRI might be warranted to gauge the severity of the injury. Like the MCL, due to this ligament being outside the joint capsule it may not be immediately treated with surgery. Doctors may advise that rest, immobilization, and progressive rehabilitation is the best option.
Meniscus

There are two menisci in each knee joint, a medial meniscus and a lateral meniscus. They are fibrocartilage, and are wedge-shaped shock-absorbing structures on top of the tibia and anchored by the coronary ligaments. The medial meniscus is more oval-shaped, and more commonly injured due to its position resisting inward caving of the knee. The lateral meniscus is more C-shaped.
There are a few different ways to classify the menisci further. One way is by the position front to back. At the front of the knee, joint is the anterior horns of the meniscus, while at the back of the knee joint are the posterior horns of the meniscus. The front portions can be damaged with hyperextension and compression, like in a locked knee landing. They can also be damaged by rapid twisting or shearing motions. The back portions can be damaged with extreme ranges of knee bending and compression, but in particular, if rotational shearing is added into the mix. The medial meniscus is commonly damaged during ‘caving’ events of the knee that also stress or tear the ACL ligament.
Another important aspect of the menisci is the inner vs outer portions. The inner portions, known as the ‘white’ zones, typically have less blood flow and are less capable of healing on their own. This tends to lead to acute injuries needing surgery to be repaired. The outer portions, known as ‘red’ zones, typically have more blood flow and are more capable of healing on their own. This tends to lead to injuries being managed with rehabilitation as the first option.
When athletes have meniscus injuries, they may have painful mechanical symptoms such as a feeling of locking, clicking, catching, or the knee joint getting “stuck”. Depending on the type of meniscus tear, athletes may lack the ability to fully bend their knee due to pain and/or swelling. With anterior horn lesions, a loss of knee extension may also be present. Another common finding for meniscus issues are joint line tenderness when palpated. There are a few other special tests, like a Thesssely and McMurray’s test, that can be used as well. Like the collateral ligaments, MRI is typically best to confirm a meniscus tear being present.
Cartilage

As touched upon earlier, the large weight-bearing surfaces of the knee joint that take high forces have extra protection. On the bottom of the femur, thick portions of firm hyaline cartilage are on top of the medial and lateral femoral condyles. This hyaline cartilage does extend around the outer surfaces of the femur, which are not weight-bearing. Often times with progressive cartilage damage, surgeries will be done that harvest pieces of cartilage from the non-weight-bearing surfaces and transfer them to the weight-bearing portions that might have damage.
The bottom portion of the main knee joint, the tibial plateau, also has cartilage that lines the top of each boney surface. Due to the high amounts of force that go through it, the menisci are additional shock absorbers against these forces, which will be covered next. This cartilage is sometimes damaged when very forceful impacts occur, particularly if in a ‘locked knee’ position.
Lastly, the backside of the knee cap also has a notable amount of cartilage. This cartilage helps to buffer against high compression forces that occur when the knee joint bends under load, and the backside of the knee cap makes contact with the “tracks” of the knee – the trochlear groove.
Layer 3 – Muscles / Tendons
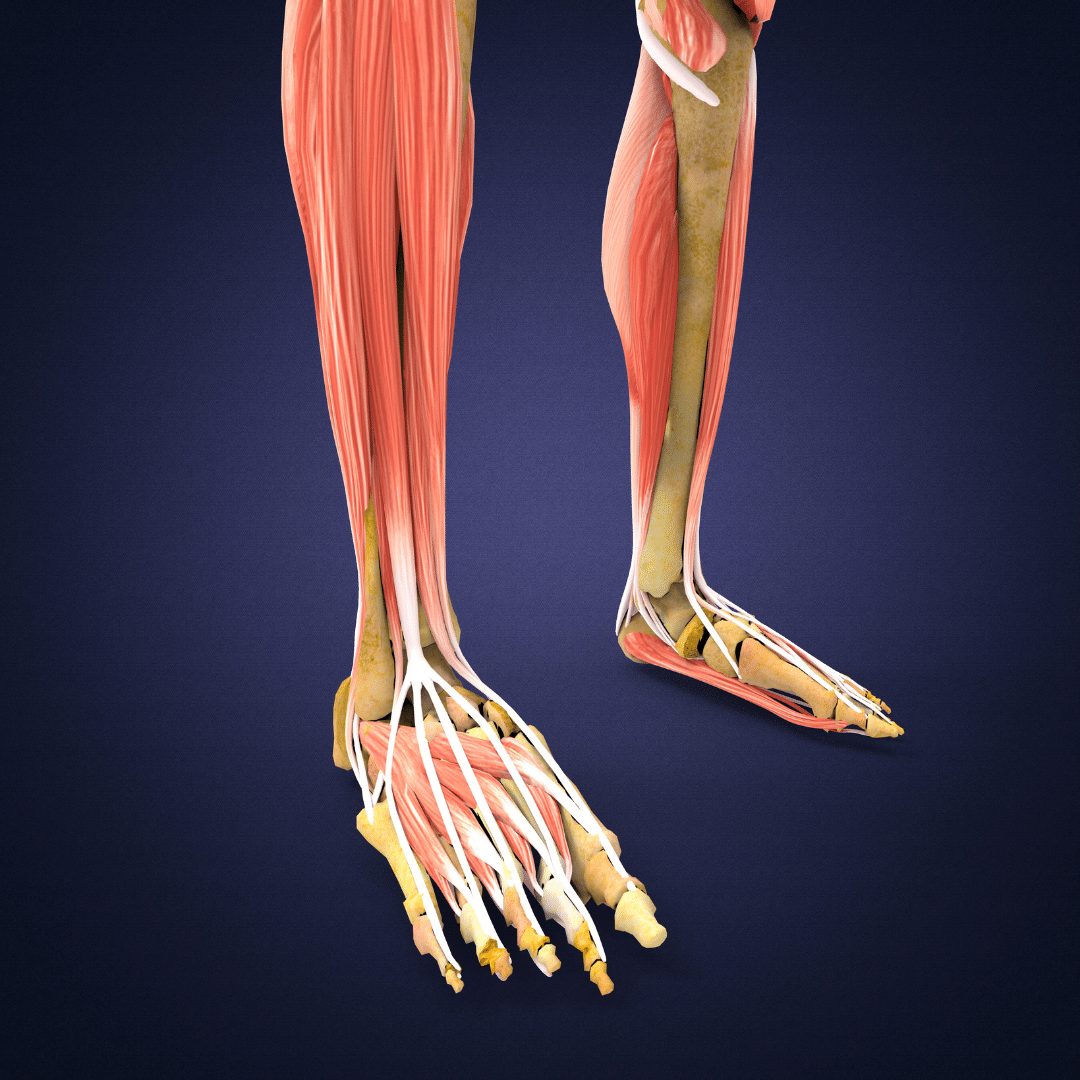
While the knee joint does possess a lot of boney and ligamentous components to support it and promote movement, it requires an enormous amount of dynamic muscular structures to function optimally. This is particularly true in relation to producing high amounts of strength/power during explosive sporting movements, but also in relation to the need to resist high rotational and side-to-side bending motions. That is where the different muscles of the high and thigh come into play. Keep in mind that the majority of these muscles span long distances, and start from the hip or pelvis. This is unlike other joints, like the ankle, where there are many very small local muscles to help control all of the joints.
Quadriceps

This muscle is made up of 4 muscles (hence quad), with 3 of them starting on the thigh bone and one starting on the front of the lower pelvis bone (the AIIS). The four individual muscles are the vastus lateralis, vastus intermedius, vastus medialis, and rectus femoris. Together, this very large muscle travels down the front of the thigh and becomes the quadriceps tendon above the kneecap. It then blends in with the retinacular tissue around the knee cap, and then finally forms the patellar tendon below the knee cap which inserts onto the top of the shin bone at the tibial tuberosity.
There is a very important, and very sensitive, fat pad as well as bursa that sit behind the patellar tendon. They both help provide cushion during high compression forces and also reduce friction as the knee cap moves. As this wild study by Scott Dye showed, the fat pad is highly sensitive and commonly may be a source of pain.
While the quad’s main role is to straighten the knee, it also has a secondary role of flexing the hip. When the foot is planted on the ground, it is crucial in both producing force for walking/running/jumping and absorbing force during landing impacts. Due to the high demand placed on it, injuries can commonly occur at different portions of the muscle. This can be true of the hip attachment of one quad muscle on a growth plate, the actual muscle itself in the middle of the thigh, the quad tendon, the patellar tendon, the fat pad, and shinbone attachment.
Hamstrings

The hamstring muscles are on the back of the leg and work in opposition to the quadriceps muscle. The 3 muscles start from the ‘butt bone’ (ischial tuberosity) on the pelvis as a large tendon, then extend down near the sciatic nerve branching out into 3 individual muscles. They are the semitendinosus, semimembranosus, and biceps femoris. They run down the length of the leg, each turning into long tendons that attach below the knee joint on the back of the shin bone.
The most important aspects of the hamstrings are the tendons themselves, and the strength relative to the quadriceps. This is because the higher tendon that all three hamstring muscles form is the subject of extremely high forces. In athletes under the age of 15, the hamstring tendon attaches directly to a large growth plate and can be the source of an injury known as an ischial apophysitis. This is also because the hamstrings are typically very undertrained in comparison to the quad muscles in gymnastics. This can lead to problems with hamstring strains, but also with a lack of strength balance around the knee joint.
Exercises like deadlifts, Romanian deadlifts, and Nordic hamstring curls are among some of the best exercises for the hamstrings based on EMG data. With gymnastics, culture continuing to be concerned about external weight usages, hamstring deficits, hamstring injuries, and ‘quad dominant’ landing patterns continue to be an issue. While there are many areas to work for knee health and performance, this is one of the biggest areas to focus on in gymnasts.
Adductors/Groin

On the inside of the knee are a variety of muscles that serve to both pull the legs together and also assist the hip in moving front to back. Towards the top of the hip, are smaller groin muscles like the pectineus and adductor brevis. In relation to the knee are the longer, more broad muscles that span from the pelvis all the way down to just above or below the knee. These are the adductor longus, gracilis, and the adductor magnus. These muscles are influential on the knee’s position in space during running, jumping, and landing. they must also work together with the outer hip muscles and glutes to create a side-to-side balance around the knee joint.
Due to the attachment of the groin muscles on the inside of the knee, it can be a common source of pain or irritation like with pes anserine bursitis. These muscles also have an influence on structures on the inside of the knee, like the MCL and the medial joint capsule. A combination of repetitive use (keeping ‘good form’ with legs together) and very explosive dynamic jumps/leaps (switch leap, switch side) can commonly lead to injuries like muscular strains. For this reason, specific caution must be taken when training high-level jumps and leaps, or when increasing impact workloads.
Iliotibial Band (ITB)
This structure is not a muscle or a tendon, but more so a very dense fascial connective issue. I wanted to include it here though, as it is commonly talked about and often misunderstood in its role in the injury. While it is possible for this structure to be painful, it is oftentimes more related to the common peroneal nerve or the capsular tissue on the outside of the knee that is the point of pain. It has been less supported that the iliotibial band being ‘tight’ causes it to snap back and forth over the outside knee bone, unless in very specific situations of instability.
With this in mind, it’s in most people’s interest to not go crazy foam rolling and crushing their IT bands. For one, we are likely not making any changes in the density of tightness or breaking up ‘scar tissue’ with any sort of self or hands-on massage work as this study and this study suggests. Second, the majority of issues that I see with the ITB are more related to workloads and strength/capacity deficits, not true flexibility.
Lastly, if notable stiffness does occur, it may have more to do with the tone of the quad, hamstring, TFL, and glute influencing it. It can be true that the outside knee structures may influence the kneecap’s position, like in patellar instability where the trochlear groove is shallow or dysplastic. That said, more work has come out supporting the idea that the femur’s position behind the knee cap, rather than the knee cap actually moving sideways by itself, should be the focus of rehab alongside great strength programs. Back to our train analogy, we may have combined problems with the train track and the train, not just a “tight IT band” yanking the train off the track sideways.
Layer 4 – Nerves & Blood Vessels
Tibial Nerve
The tibial nerve is the main nerve that runs down the back of the knee joint, alongside the other blood vessels in the popliteal fossa. While it does not have a major role in common injuries, it is worth mentioning due to it sometimes being damaged with knee hyperextension injuries. When these injuries occur that may damage the tibial nerve or blood vessels in the back of the knee, it is absolutely crucial that the athlete gets to the Emergency Room/Hospital ASAP to prevent serious complications from occurring.
Common Peronneal Nerve
Another nerve worth noting is the common peroneal nerve, which runs on the outside of the knee joint and down into the lower shin bone. Due to it’s location along the knee joint and near the iliotibial band, it is thought to be a common pain generator on the outside knee. This often occurs with instances of repetitive knee bending and landing, like running or biking.
Layer 5 – Kinetic Chain
Looking just at the knee joint without consideration to the entire leg is one of the most common mistakes sometimes made. As I hope has been made clear, the knee joint is massively influenced by the core/hip joint above and ankle joint below. Remember that the ‘train tracks’ themselves can twist and move based on what these two areas are doing.
Core & Hip Joint
We must remember that the lower back/core and the hip joint are inseparable. Due to this, they both have a direct impact on the knee joint through a ‘top down’ influence. As has been suggested in studies, an over-arched lower back posture (anterior pelvis tilt) may create more inward motion of the hip joint (internal rotation). This inward motion then directly affects the position of the knee joint, moving it into a ‘knee cave’ position (dynamic valgus). So, if the hip joint lacks strength, coordination, or control, it is very possible for the knee to be put into a less optimal position to produce and absorb force.
While there are many muscles in the hip that can help here, the main ones in relation to the knee are the glutes and the hip rotators. The gluteus maximus extends the hip, but also is hugely important in absorbing impact forces with the hamstrings during proper squat motions. The gluteus minimus and medius serve to raise the leg outward but also have a crucial role in maintaining an even pelvis position during single-leg activities like walking, running, and landing. The deep hip rotators help to rotate the knee outward into external rotation, which is in opposition to the ‘knee cave’ position that is concerning for ACL, MCL, and meniscus stress.
Now, this being said it isn’t an automatic connection that having weakness in the hip joint ’causes’ knee pain. There is actually evidence showing that those with knee pain may actually have stronger hips. It could be that knee pain develops, and then hip weakness comes up as a secondary effect. A bit whacky I know, but the literature is mixed here. There is actually evidence that those with knee pain may actually have quadriceps weakness. So, maybe it’s more about having the appropriate capacity of the muscles directly controlling the knee, and as a result the quad/patellar tendon, that is key here.
For both the hip and the knee, these muscles also must be a centerpiece of our training programs if we want to develop the most explosive power and excellent skill technique possible. We want to develop overall leg strength, but also consider how the hip works with the knee to not put someone in really disadvantageous positions during landing like a big knee cave under high force which might stress the ACL.
Ankle Joint
The foot and ankle, on the other hand, exert a ‘bottom up’ influence on the knee joint. There are a few factors here. One of which is ankle mobility, which when limited can change the knee’s position. If the ankle lacks a toes-up motion of dorsiflexion, it may cause the foot to spin outward or the foot to flatten during impact. Both of these things may cause the knee to drift inward into the same ‘knee cave’ position above that isn’t ideal.
Another common compensation for limited ankle mobility is the heel rising off the floor during impact, with the weight shifting more into the ball of the foot. As a result, this shifts more of the force on the knee to the structures on the front of the knee (knee cap, patellar tendon, fat pad, quad tendon, etc) and makes it harder for the hamstrings and glutes to share the load. These issues are very common in gymnastics, possibly contributing to high rates of pain on the front and inside of the knee joint when high impact forces, high repetitions, and high workloads exist.
While mobility is the most common issue from the ankle that negatively impacts the knee, strength and control issues are also important to address. The calf muscles, the gastroc, and soleus play a huge role in helping to absorb forces during landings that help reduce the risk of ACL injuries (more here and here). The muscles within the ankle and foot that support/maintain the arch during impact are also crucial. If they are not strong enough to maintain a good arch shape, and supportive foot posture, an excessively flat foot position may lead to a similar inward position of the knee point during jumping or impact. While these things don’t mean someone will automatically have an injury, they have been noted risk factors within the scientific literature.
What Are The Most Common Knee Injuries in Gymnastics?
Now that we have reviewed the background concepts, factors that may be contributing to injury, and the underlying anatomy, it’s time to talk about specific injuries. While there are a massive amount of injuries that occur in the knee joint, I will focus primarily on those that are most common in gymnastics. We will start with the most common and biggest categories first based upon the research noted above, and then work our way down into more nuanced injuries.
Patellofemoral Joint Pain
As mentioned in the introduction, “patellofemoral pain” or “PFJ pain” is a wildly helpful diagnosis. It essentially says someone has knee pain but does not share further insight into why some has that knee pain, or what to do about it. In the early 2000’s more science emerged discussing this concerning problem and offering more specific diagnostics. You can find some great research papers here, here, and here.
Two of my good friends and mentors, Mike Reinold and Lenny Macrina, were at the forefront of this area of research being mentored by Kevin Wilk (his classic paper here). As a result, I’ve been very fortunate to learn from them and apply both their ideas and the larger scientific communities ideas to the gymnastics world. Here are some of the more common subsets of PF pain that I commonly see in gymnasts, continuing with our ‘train and train tracks’ analogy to help connect the dots.
Excessive Lateral Pressure Syndrome (ELPS)
ELPS stands for Excessive Lateral Pressure Syndrome. People tend to have pain on the outside portion of their knee, and also may have some global achiness and soreness around their knee cap. It typically occurs with bending of the knee or repetitive impact. In a broad sense, irritation typically occurs because the outside portion of the kneecap is experiencing excessive amounts of contact with the bones underneath it. The outside portion of the “train” is pushing hard into the outside “train track” leading to pain, irritation, and possible tissue damage.
The main theory behind why this occurs used to be that excessive tightness of the iliotibial band, and weakness of a portion of the inside quad muscled (the VMO or Vastus Medialis Oblique) was causing the knee cap to be pulled off to the side. With this theory in mind, many people thought that the knee cap needed to be pulled back towards the middle of the knee joint. Things like McConnell taping, repositioning buttress braces, targeted aggressive IT band soft tissue work, and VMO specific strengthening exercises like short arc quads were the mainstays of rehabilitation. Then, if someone didn’t see improvements, more drastic measures like Iliotibial Band Release surgeries were used.
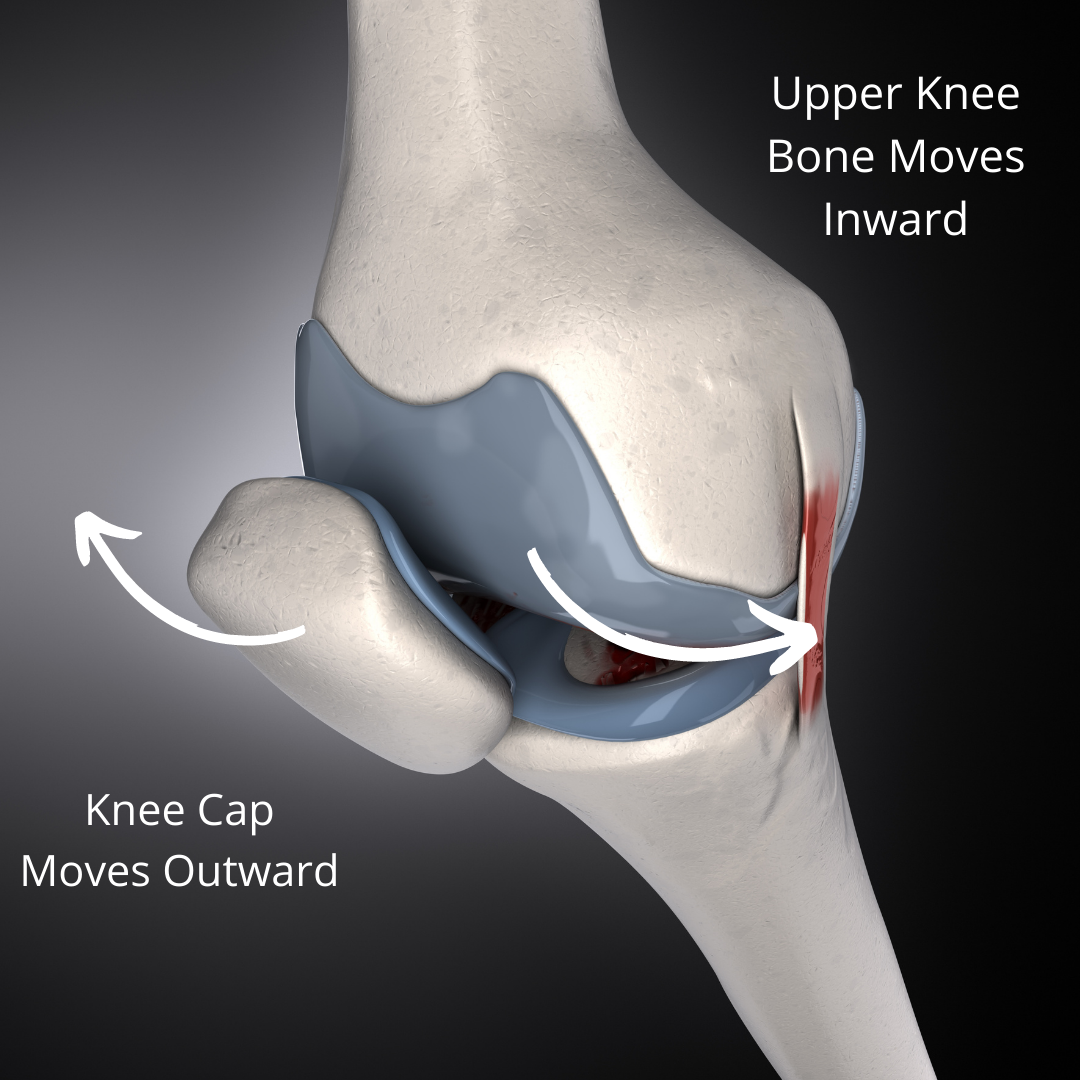
Based on new research (more here, and here) in the last 20 years, the thoughts around ELPS have changed quite a bit. As mentioned, one of the biggest findings was by Chris Powers related to the hip’s role in the position of the femur behind the knee cap. During research, it was found under dynamic MRI that it may not be the “train” that is sliding off the track outward, but more the “train track” sliding inward relative to the train. Essentially, if someone lacks the strength and capacity to maintain good alignment of the knee joint, the outside portion of the femur (femoral condyle) may be making repetitive contact with the backside of the knee cap surface (medial facet of retropatellar cartilage).
This may be due to flexibility issues at the ankle/hip joint, strength deficits of the quads and hamstrings locally at the knee joint, strength deficits at the hip, or control and fatigue issues globally in the leg. These are all issues that may create this type of knee pain, and many more below. Once this was investigated, things started to get much more complex in terms of evaluation and rehabilitation, but also made more sense. Rather than trying to focus on repositioning the kneecap and very hyperfocused VMO strength, the new science lends itself to focusing on the more global high-level knee and leg strength, jumping and landing mechanics, looking at the entire kinetic chain, and workload management of hard impacts.
Medial Gapping
This is a very similar situation to the ELPS type of knee injury noted above, with the difference being that these athletes typically feel pain on the inside portion of their kneecap. They can also feel the strain on the lower/inside part of their knee joint itself. The most prominent theory here is that the same dynamic motion of the upper thigh bone, the femur, rotating inward behind the knee cap can cause excessive stretching of the structures on the inside of the knee.
It’s hard to know exactly what may be referring to pain in these athletes. But some structures involved may be the medial retinacular tissue, the medial joint capsule, the MCL, or the MPFL. Typically these gymnasts complain of soreness on the inside of their knee with running, jumping, landing, and squatting. Sometimes it is very evident to see a more dramatic “knee cave” known as dynamic valgus during impact. In other athletes, it’s less subtle or happens rapidly so it is hard to detect. Tests like a medial gapping valgus test, or a step-down test, can be used to see if irritation occurs on the inside of the knee reproducing pain.
In these situations, a combination of impact workload modification, education about proper jumping/landing technique, and building quad/hamstring leg strength is the first line of help. Beyond this, checking for limited ankle mobility can be useful. If a gymnast has a very stiff ankle joint, it may drive the foot to over-flatten with the arch collapsing and creating inward motion at the knee joint which might create pain. In some cases, but not all, a hip strengthening program might be useful as well. This is usually best implemented if specific strength testing with a dynamometer shows a noticeable strength deficit. Lastly, at some point, direct strengthening of the inside of the knee, with exercises like adduction raises and then Coppehnagen side plank progressions, can help rebuild tissue capacity.
Global Compression
In the global compression subtype of patellofemoral pain, the kneecap itself tends to be pressing down on the bones underneath it during bending. You can think about this picture as the ‘train’ in our analogy pushing down very heavily on the ‘train tracks’ as it tries to move up and down. What tends to happen is that this creates excessive press on both the backside of the knee cap and also the bones that the knee cap sits on.
There are typically a few contributing factors to this. One is that there may be an excessively high amount of jumping and landing happening in a short period of time, causing a certain part of the back of the knee cap to keep getting irritated over and over. Another factor may be excessively stiff quadriceps muscles, which may be creating lots of pressure down onto the kneecap as a gymnast lands.
Also, the gymnast may be landing in a ‘quad dominant’ landing pattern, which involves an upright torso, limited knee bend, and the knees/feet together. While many are taught to use this landing strategy, it may not be ideal to help spread forces out to another area of the leg like the hamstrings, glutes, calves, and core.
A Thomas test can be used to help see if someone has excessively stiff quads. Double and single-leg squatting progressions, or step down tests, can be used to also determine if the pain is reproduced as the knee bends more. The deeper the knee bend, the more compression occurs in the knee joint. If someone complains of pain around their knee cap globally or feels a sensation of pain ‘deep’ in their knee behind the knee cap, it may indicate global compression syndrome.
A combination of temporarily reducing impact workloads, changing strength exercises from things like deep squats to step-ups or split squats, foam rolling or soft tissue to the quads, stretching the quads, and eccentric exercises to the quads like split squats, are my go to’s first. Then, a slow reintroduction to squatting, jumping, and landing can be done moving from soft surfaces to hard surfaces.
Patellar Instability
This type of knee pain tends to occur in athletes who are naturally more hypermobile, or who have generalized lots of joint laxity. Due to this, the ligaments and joint capsules that support the knee, and help maintain its position during movement are a bit more loose. This is not inherently a bad thing, as many high-level athletes like gymnasts are great at their sport due to this genetic makeup.
As mentioned in the anatomy section, the “train” (patella) sits on the “train tracks” (trochlear groove of the femur and tibia) with only a little bit of inherent boney support. The back of the knee cap is more of a rounded shape, which does allow it to sit snuggly inside the grove made by the two knee joint bones. But, without supporting structures like ligaments and muscles, it can easily slide out of place. This is where structures like the MPFL (medial patellofemoral ligament), patellar retinaculum, Iliotibial band, and other ligaments come in. More research on that here and here.
It’s also why good alignment of the knee with the hip and ankle is important during high force movements. This alignment of these joints during these movements helps keep the patella from sliding out of place. If the knee cap is just moving around a lot and creating tissue irritation or bone bruising, it is referred to as patellar instability. If the knee cap actually pops outside the knee joint groove, and then quickly pops back in, this is referred to as a pateallar subluxation. And lastly, if the knee cap pops outside the knee joint groove, and then stays out, this is referred to as a patellar dislocation.
During all of these situations, there is some degree of tissue irritation as oftentimes the stabilizing structures are stretched out. There can also be bone bruising or cartilage irritation that occurs on the backside of the patella, or the outside of the knee joint groove during the instability. With patellar instability or less severe cases of subluxation, typically a course of rest, rehabilitation, and strength work is the main approach. This is in an effort to calm down the knee, increase strength of the quads/hamstrings/hips, correct any concerning movement patterns, and resolve pain.
With more severe cases of reoccurring patellar subluxation or dislocation, surgery may be warranted. For one, repetitive events of instability may create bone and cartilage damage that may need to be repaired. In many cases, the MPFL may be damaged, or there may need to be debridement of the joint. Sometimes the MPFL may be torn and in need of repair. Lastly, with people who may have unique anatomy like a shallow knee joint groove, excessively lose ligament support, or less than the favorable alignment of their shin bone, surgeons may change these things to add more inherent stability.
Fat Pad Irritation / Bursitis

Just behind the knee cap sits two structures that are very common sources of pain in gymnasts who undergo lots of impacts. One is the fat pad, which serves to help absorb forces between the kneecap and knee joint bones during bending. As mentioned in the study by Dye, it can be one of the most sensitive structures in the knee and commonly produce pain. The second structure is the prepatellar bursa. Bursas are small, fluid-filled sacs that help to reduce friction points that experience lots of bending or rubbing. In this case, it also serves to help prevent excessive friction on the front of the kneecap as the skin and soft tissues glide over it. There are also important bursas above the knee cap around the quad tendon, and below the kneecap around the patellar tendon. More research on that here and here.
Due to their proximity to each other, and them commonly being irritated by similar movements, they tend to be overlapping in diagnosis. It’s often challenging to know for sure which structure is the main source of someone’s pain. Pain is typically felt on the front or just below the knee cap, in the small spaces outside the patellar tendon. With the two bursa’s above and below the knee cap, typically pain is a bit more localized to those spots of the quad tendon or upper shin bone.
With this in mind, the fat paid is typically more irritable with repetitive jumping, landing, and high compression forces. A fat pad impingement test (Hoffa’s Test) can be used if this is a suspected source of someone’s pain. Another version of the test where a medical provider squeezes the fat pad and attempts to lift it out of the joint space during knee extension can also be used. For bursa irritation, direct palpation over the areas may produce pain. Bursa irritation and swelling near the surface of the skin is also commonly seen, sometimes with notable fluid increases. For both of these conditions, imaging like MRI can confirm what’s going on. As with many of the types of knee pain above, a combination of rest from impact, teaching proper landing mechanics, progressive leg/knee strength work, and a gradual return to sports will be important.
“IT Band Syndrome” or Possible Common Tibial Nerve Irritation

I wanted to include this type of patellofemoral pain as there has been a change in thought for its cause over the last 10 years (research here and here). This is usually pain on the outside of the knee that occurs with repetitive impact, knee bending, or going downstairs. It was once thought that the Iliotibial Band being very tight was causing the end of the Iliotibial band near the outside of the knee joint to ‘pop’ back and force over the outer knee bone. The main idea was that because of this stiffness, and repetitive popping effect, the Iliotibial band became inflamed causing outer knee pain. Working off this theory, many people (including my old self) would recommend very aggressive IT band foam rolling or soft tissue work, along with other methods to ‘release’ the IT band.
Due to new research in anatomical studies, fascial density, and running injuries, we are finding this may not be the case. For one, it is now suspected that the common tibial nerve sitting near the outer knee joint and IT band may be the more irritable structure. It could be that the repetitive motions, and improper workload ratios, are creating this nerve to become aggravated. It also may be that if we want to make changes in pressure on this nerve, we may want to focus more on muscular flexibility that influences the IT band (quads, hamstrings, TFL, glutes) and not the very dense IT band tissue itself that likely can’t be changed with soft tissue work. So now when these types of injuries present themselves, I am typically not recommending as much soft tissue work to the IT band and instead activity modification, strength work, and ways to reduce irritation on the nerve during sports.
Plica Irritation
A plica refers to a small fold of capsular tissue around a joint that helps serve as extra protection. We have many of these throughout our bodies, and they can sometimes become a source of pain if they get pressure put on them during sports or repetitive motions. While the are 4 around the knee joint, the plica on the inside of the knee tends to give people the most trouble. Pain, and sometimes a popping or clicking sensation, can occur with bending, landing, jumping, or other activities. These tend to be a bit more challenging to diagnose, and either a process of elimination or MRI is the most common way to sort this out.
Growth Plate Injuries
Osgood Schlatters
There are two main growth plate injuries that tend to occur in gymnasts. The first, and more common, is Osgood Schlatters. This is when the growth plate of the upper shinbone where the patellar tendon (from the large quad muscle) attaches. Growth plates are not fully formed bones. They are more made up of softer, spongy bone. As a result, they are not quite equipped to handle really high forces, in really high amounts. More on this via research here and here.

This oftentimes creates a problem for young gymnasts, who are not yet fully matured but are doing very high force impacts. It is possible for this growth plate to remain open until the age of 14-16 in some cases. To make things more challenging, high amounts of traction force that occur when a young gymnast is growing puts more force on these growth plates. The long bones of the shin and upper thigh grow at a much faster rate than the muscles and tendons can keep up with, creating high amounts of pulling during impact.
It is this combination of factors that often leads to pain at the top of the shin, which is due to bone inflammation. Contrary to what some may suggest in gymnastics culture, this is not something to just ‘work through’ or something that is ‘just part of gymnastics’. If pain is ignored, and proper rest/care is not given, it is possible to see a growth plate irritation turn into a growth plate stress fracture. This is a much more serious condition and often requires extended periods of time away from gymnastics to let it heal.
When someone has a flare-up of Osgood Schlatters, I first recommend to them that they plan for 2-4 weeks of reduced or no impact. This is required to help the bone inflammation resolve. Then, efforts can be made to reduce pain or swelling by using compression, elevation, and movement to tolerance. Sometimes patellar tendon straps can be useful to take tension of the painful area, but please keep in mind these should not be used as a “quick fix” and way for gymnasts to just keep training. In my experience, doing this just compounds the issue and makes things worse down the road.
Soft tissue work to the quads and calves via hands-on massage, light stretching, and light foam rolling can also be helpful in the first few weeks. After pain reduces, local strength work should be done to help rebuild the bone’s capacity and tolerance for load. I typically suggest starting with a combination of closed chain exercises (hip lifts, half squats, step-ups, lunges) and open-chain exercises (knee extensions).
It is extremely important that gymnasts reintroduce impact-based exercises first in rehab (pogo hops, scissor hops, skipping, running, box jumps, etc) to set them up for success. After a few weeks of this 3x/week that doesn’t increase pain, I have gymnasts start back on softer surfaces like a trampoline and Tumbl Trak 3x/week while continuing their strength work. Then if they continue to feel good, they can slowly ramp up to medium impact surfaces like rod strips and then finally hard surfaces like floor/vault/beam. If this slow progression isn’t respected (yes, even in the middle of meet season) gymnasts can struggle for years being limited by this.
Sinding-Larsen-Johansson Syndrome
This growth plate condition is not as commonly seen, but can sometimes be an issue in gymnasts. This refers to growth plate inflammation of the lower tip of the knee cap, called the inferior pole. As mentioned in the anatomy section, during the first 20-30 degrees of knee bending, the bottom of the knee cap is what makes contact with the underlying bones. This is also the same location for the start of the patellar tendon which bridges down and attaches to the shin bone.
It is this combination of factors that may cause a gymnast to feel pain at the bottom area of their kneecap during running, jumping, and landing. Although the location of pain may be slightly different, the exact same approach can be taken for this as for Osgood Schlatters. I recommend people follow similar advice as offered above.
“Internal Derangements”
This is another doozie of a term seen in my research studies, as there are a ton of different possible issues that can fall under this category. To not bore people during these next sections, if you are looking for research please refer to the links below for useful papers.
- ACL – here, here, and here
- MCL – here, here, and here
- PCL – here and here
- LCL – here and here
- Meniscus – here, here, and here
There are some common factors to treating various internal derangements of the knee. In all cases, there will be some degree of pain, swelling, and range of motion loss that needs to be addressed. This will be covered during the ‘4 phases of rehab’ section below.
That said, the reality is that due to the different functions of these structures within the knee they have different mechanisms of injuries, different treatment continuums, and different treatment needs. I will review some of these key components for the most common types of knee internal derangements, moving from the most common to the least common.
It bears repeating that for the main cruciate ligaments (ACL, PCL, MCL, LCL) there is a range of severity in injuries. In A Grade I sprain, the ligament is stretched and irritated, but microlearning does not occur. While it can still create swelling and pain that limits sports participation, typically it only requires 4-6 weeks to see good healing.
In Grade II tears, more damage occurs as the ligament is overstretched to the point where micro-tearing occurs. This leads to much more pain, swelling, and tissue damage. Visible bruising or enlargement of the knee is seen, and most athletes have to modify their walking with crutches or a brace for a period of time. Depending on the ligament damage, surgery may be required.
The ACL and PCL for example, are within the knee joint capsule and have less direct blood flow as well as less inherent healing capacity. They are also more primary in their role to help the knee during bending or straightening. When Grade II tears occur, a surgical repair that uses a graft (quad, patellar tendon, hamstring tendon, etc) is typically opted for in athletes to reduce the risk of further injury. The MCL and LCL, on the other hand, are outside of the knee joint capsule and get much better blood flow that predisposes more healing capacity. Oftentimes, surgeons will recommend a period of rest, bracing, restriction range of motion, and rehabilitation while allowing the ligament to scar down and heal.
Unfortunately, there are times when the high forces of gymnastics landings will fully tear the ligament. These are Grade III injuries. They tend to be the hardest to deal with, as they come with notable tissue damage, pain, swelling, and interference with movement. They most often require surgery and extensive periods of rehabilitation following repair or reconstruction. While I will break these injuries out below for the sake of learning, keep in mind that due to the very high impact forces of gymnastics, there may be times when multiple ligaments or multiple structures are damaged. These create very complex, unique situations, and must be taken on a case-by-case basis with a great team of medical providers all working together.
ACL Injuries
ACL injuries are by far and away one of the most common and discussed knee injuries in gymnastics. This is not only due to how often they occur, particularly in females, but also due to their devastating consequences on gymnastics performance. The most common mechanism for ACL injust is landing with a sudden inward cave of and twisting/pivoting motion under high force. This injury can also occur with a ‘lock legged’ landing that forces the knee into hyper extension.

Typically, athletes feel a distinct ‘pop’ and buckling of their knee, which then results in swelling, stiffness, difficulty moving the knee, and pain. Sometimes athletes are able to walk, albeit not comfortably. Hands-on special tests like a Lachman test, Anterior Drawer test, and Pivot Shift test can be used to rule in the suspicion of a full ACL tear, and often an MRI will be warranted to get conclusive evidence.
Female athletes are at a higher risk of injury due to a wide array of factors (outlined in this study well) ranging from genetics, to laxity, to hip width, to hormonal influences, and more. As research suggests, two of the biggest modifiable factors to reduce the risk of ACL injuries, particularly in female athletes, are using proper landing patterns and using high-level science-based strength and conditioning programs. There are some fantastic research papers reviewing the main mechanisms and current approaches to treating ACL tears (more here and here).
While there are many key points to ACL rehab following surgery, one is restoring knee extension early and trying to gain symmetry (even some hyperextension) between sides. As this study and others have suggested, regaining full motion is correlated with more favorable outcomes. A second key point of ACL rehab is vert, very high levels of strength are being restored. There is evidence that long-term quad and hamstring weakness may be present up to a year following surgery. The addition of certain exercises may vary based on the type of graft someone has (quad vs patellar vs hamstring graft…cadaver grafts falling out of fashion) but regardless it’s crucial that strength is a priority.
This is a must-have for both early and late rehab. Swelling management through compression and regular exercise along with tools like Blood Flow Restriction (BFR) and Neuromuscular Electrical Stimulation (NMES) are great ways to build strength immediately postoperatively. There is fantastic research here, here, and here on these tools for ACL rehab. In the mid to late stages of rehabilitation, more formal and traditional strength and conditioning methods must be used. This includes not only following periodization methods to make rehabilitation hard enough but also using the main movement patterns in a holistic program including the squat, hinge, split pelvis, single-leg, carries, and lateral motions. This encourages a well-balanced strength profile. Filling in lots of accessory work (core, outer hips, calf strength) and dynamic stability work (single leg and reactive balance) is also key.
Lastly, in the late stages of rehabilitation, we really want to develop power, speed, plyometrics, and overall cardiovascular capacity. We are seeing that it really may take 9-12 months to fully rebuild an athlete’s capacity, and return them to above baseline levels of strength/power to get back to gymnastics. The use of various jumps, med ball exercises, sprinting drills, and proper double/single-leg landing mechanics must be taught. Then, a slow, graded return to gymnastics program over 6-8 weeks (more below) is the final step for ACL injuries, followed b continued high-level strength and maintenance care.
MCL Injuries
The MCL is another commonly injured ligament in gymnastics. An isolated MCL injury sometimes happens when someone had a force that pushes their knee directly inward, creating strain on the ligament. This typically produces notable pain on the inside of the knee, swelling, difficulty bending the knee, and in many cases challenges with walking/stair climbing. Due to the position of the MCL, it is also very common for it to be injured in combination with the ACL during the rapid ‘knee cave’ type mechanism mentioned above. As the knee twists or pivots inward, the MCL can be rapidly stretched or twisted creating injury.
As mentioned above, the MCL is different than the ACL/PCL in that it is located outside the knee joint. This creates a situation where it has much more blood flow, and thus a potential to heal than the ACL/PCL located inside the knee joint. For this reason, it is very common to hear about Grade I and Grade II injuries being managed with activity modification, rehabilitation, and possible bracing to assist with pain/swelling management. While it does require more time in some cases, many physicians will give gymnasts a brace that restricts motion and crutches for 4 weeks in an effort to help the MCL heal and scar down. Then, with progressive exercises and weaning off the brace/crutches, the ligament’s tolerance to load can be rebuilt. In Grade III injuries, that fully tear the MCL, surgery is warranted to help repair the natural anatomy.
With MCL injuries, it’s important to remember that progressive degrees of bending may stress it during the healing process. For this reason, we must be careful with our range of motion progressions and mobility work so we don’t create tissue inflammation. Also, it’s crucial to remember that adductor muscles also have an influence on the MCL bands and may indirectly create soreness if used a lot. For this reason, I’m typically very cautious about medial straight leg raises in the early parts of rehab as well as Copenhagen lifts in the late parts of rehab. When added in with the right doses, and at the right time, they are beneficial. But, we must be careful and communicate about symptom levels.
Meniscus Tear Injuries
Different Meniscus Tear Factors
Meniscus tears encompass a very wide range of possible injuries ranging from mild irritations to degenerative tears, to large acute tears. Remember that each knee joint has both a medial and lateral meniscus. The medial meniscus is more commonly injured, as like the MCL it is in a position to be stressed under ‘knee cave’ incidents. A combined injury to the ACL, MCL, and the medial meniscus is referred to as the “Unhappy Triad”. In order to understand the type of meniscus tear, and as a result the best treatment options, it’s important to remember how the location, duration, and type of tear all play a role.
First, the location of a meniscus tear influences the types of motions that may be impacted. The front portion of the meniscus (called the anterior horns) tends to be more stressed when the knee is straightened or hyperextended position. This is why landing “lock legged” or having hyperextension impact events may cause a tear to this portion of the meniscus. Due to how often gymnasts straighten their knees and rebound in stiff-legged positions, these can be problematic for gymnasts.
The middle portions of the meniscus tend to be more stressed when the knee is in the middle range of bending. Again, due to the high impact forces of landing and many twisting/pivoting skills in gymnastics, there are many meniscus tears that occur in this part of the knee joint.
The back portions of the meniscus (called the posterior horns) tend to be more stressed with much deeper degrees of knee bending (think deep squatting). Gymnastics can be done with modifications as to not put tons of pressure on this area of the meniscus, so it is possible to have better outcomes when tears are located here. This is with the exception of a Root Tear, which involves a piece of bone the meniscus attaches to being pulled off. These are more complex injuries and are almost always managed surgically.
Second, the location of a meniscus tear also influences its potential for healing. Remember that different areas of the meniscus receive different levels of blood flow, and as a result, may have very different capacities for healing. The outer portion of the meniscus (called the ‘red zone’) has much more blood flow. Smaller meniscus tears, or less complex tears, located in this area may have a better potential to heal with rehabilitation and activity modification. The next central part of the meniscus (called the ‘red-white’ zone) has a bit less blood flow.
The most inner portion of the meniscus (called the ‘white zone’) has the least amount of blood flow. So, when tears occur in these two more inner zones, there may be less chance for them to heal on their own. Also due to their position, they may cause problems getting caught in the joint space creating pain/swelling as well as mechanical symptoms like catching, locking, and the knee getting ‘stuck’. Due to this, many times surgery is warranted to help repair the tissue and restore the normal anatomy.

Third, the duration or acuity of a meniscus tear may change its potential to be managed with or without surgery. While most of the research is done in older individuals, there is evidence that degenerative and slower developing, long-term meniscus tears may not have great outcomes with surgery. They may be present on MRI, and cause some issues, but may not be the main source of someone’s pain. This is in contrast to rapid onset, acute meniscus tears that usually occur with some sort of trauma. These tears tend to create much more tissue damage and are more involved. These tend to be tears that people really struggle with if not repaired or debrided through surgery.
Lastly, the type of meniscus tear (often linked to duration) must be considered. There is a wide range of different meniscus tears, due to the many different forces that go through the knee joint. Some tears are more slow and degenerative in nature, so they tend to have small lesions with fraying of the meniscus. Some tears (bucket-handle tears, flap tears) may be caused by high force impact and as a result, produce large chunks of tissue damage that may be floating within the knee joint. As mentioned, due to their involvement they may require surgery for better outcomes. Lastly, some tears (radial and horizontal tears) are caused by more rotational and shearing forces seen in sports. These may have a more case-by-case nature to them on the best course of action. Complex tears are probably the most challenging of all, as the tissue involved can be variable and possess different angles and movement impairments.
Meniscus Surgery/Rehab Trends
In general, if surgery is warranted more surgeons are suggesting to preserve meniscus tissue whenever possible through a meniscal repair as compared to older thoughts of removing the damaged tissue through a meniscectomy. This is because there is concern that by removing the meniscus tissue, the compression and loading forces through the knee have less surface area to be spread out across. There is also a concern that the underlying cartilage may start to become the focal point for force, which then leads to much bigger headaches.
Rehabilitation for meniscus injuries, both surgical and nonsurgical, tends to require some sort of deloading, bracing, and progressive exercise program. There is a lot of variability in periods of being no weight-bearing. Part of this is surgeon preference, with some being more conservative and wanting to not stress the healing tissue. Others are less conservative, using the theory being weight-bearing as tolerated allows hoop stresses within the meniscus to aid in healing. Another cause of high variability is the type and severity of tears. Smaller, less involved tears may not need prolonged time away from weight-bearing. Larger, more complex tears may need notable time to heal and may require 6 weeks of non-weight-bearing.
Regardless of weight-bearing status, all meniscus injuries will need a lot of focus on swelling management, progressive gains in range of motion, and strength work. It is worth noting that sometimes we must be cautious with hamstring-specific exercises for tears involving the posterior horns of the meniscus, as the hamstrings do have capsular attachments that might tug on the meniscus. Just as with hamstring ACL graphs, caution might be warranted for the first 6 weeks. Impact forces tend to be delayed up until 3 months, starting with jogging, to help protect the healing tissue. Then lastly, more advanced strength work and sporting motions tend to progress over a few months, with most people starting to get back to sports in the 5-6 month range.
PCL Injuries
These injuries are typically suspected when someone does have a unique hyperextension injury with their knee rotating back/outward in a fast motion. Again, sometimes a ‘pop’ may be heard or felt, leading to swelling, pain, and limited motion. Hands-on special tests like a Posterior Sag/Step Off Sign and a Posterior Drawer Tests can be used to determine if someone may have a PCL tear. From there, MRI can again be used to get conclusive evidence about the status of the PCL.
Most often times, Grade I PCL strains are just managed with appropriate rest, strength work, and trying to protect the area. Grade II strains that result in a decent amount of tissue damage, or laxity that brings about more problems, may be dealt with via surgical reconstruction. Grade III PCL tears are almost always reconstructed unless there are certain circumstances, as being deficient in this ligament can give way to further tissue damage or instability.
LCL Injuries
As mentioned in the anatomy section, due to a lack of direct contact in gymnastics between athletes, LCL injuries don’t happen as often. That said, there are times when landing twisting elements incompletely, or if the body is tilted over the knee in a certain way, an outward ‘varus’ force can occur at the knee. That could create a situation where the LCL is strained or torn. Some very unique types of accidents or landings might also damage what is called the Posterior Lateral Corner of the knee, creating a situation of specific care or surgical management.
As with the MCL, many times conservative management is done due to the LCL’s blood flow and healing potential. A period of bracing, limited weight-bearing or range of motion, and specific strength work may be the better option over surgery. Just as adductor loading and Copenhagens may be something of caution in the MCL, abduction leg lifts and side planks may be something to hold off on until the ligament heals fully. These types of movements might stress the outer side of the knee if applied too soon, creating soreness.
Tendinopathies
Moving more into the “overuse” category of knee injuries in fully developed, I will now cover tendinopathies. Interestingly, I think that many of the same factors that contribute to growth plate injuries in youth gymnasts are the same factors that contribute to tendinopathies/tendon ruptures in older gymnasts. It is my thought that as gymnasts mature, the growth plate no longer becomes the main vulnerable point, and instead, the tendons themselves take the brunt of the force. This may lead to progressive degeneration, tendon makeup changes, and pain or pathology.

In the bigger picture, it’s helpful to follow Jill Cook’s work here and view tendon issues as existing on a continuum. This paper, this paper, and this paper are great to read and are what the following sections are based on.
Tendonitis
On the left side of the continuum, you have the very acute and ‘hot’ tendon injuries, often called tendonitis. This typically occurs in a single incident or tipping point of pain, bringing on sudden very intense bouts of pain. In most cases, this typically has a true inflammatory component as the tissue is suddenly overloaded with a high force movement or some sort of sudden load spike.
Tendonopathy
In the middle of the continuum are tendinopathies. The role of true inflammation has been combatted in the current research, and it is mainly thought not that an imbalance of workload placed on the tendon, and the tendons lacking the capacity to handle it, create a progressive degenerative process within it. This could be due to the excessive workload being placed on it without enough recovery between loading bout (lots of sudden impacts in a few weeks/ months time). It could also be related to a lack of strength, making the tendon less able to tolerate high forces.
There also may be other factors like nutrition status, technique, genetics, unique anatomy, and more. Given all this, what is typically happening here is that the tendon itself starts to change, and the tissue that makes up the tendon (collagen) starts to become not the healthiest type that is able to handle the load. This could create a situation where the nerve ends start to grow in the tendon creating pain, or that due to its lowered capacity to handle the load, high force impacts or over-stretching of the tendon can cause microdamage and irritation. To help address this, typically a reduction in tendon stress is needed for a short period of time while exercises and strength drills can be used to increase the tendon’s capacity and possibly promote healthier collagen tissue to remodel.
Tendon Rupture
At the far right side of the continuum would be tendon failure, also referred to as tendon ‘ruptures’ or ‘tears’. This is a very devastating situation, where the tendon has gone through so many cycles of microtrauma or degeneration, that in one moment of tissue overload the tendon reaches its failure point. These injuries are much more devastating, requiring surgery to repair the tissue, extended time away from gymnastics to rehab, and a gradual return to sport progression being used. Not to mention, it dramatically impacts the athlete’s mental health and performance for the rest of their career.
Thankfully, patellar tendon and quad tendon ruptures are less common in gymnastics. That said, knowing these issues exist, it’s crucial for people in gymnastics to look at the entire spectrum of tendon issues from the younger ages all the way to the later ages, and consider what can be done to mitigate excessive damage from occurring.
Patellar /Quadriceps Tendinopathy
The most common tendon issue that gymnasts struggle with is patellar tendinopathy. The same types of factors typically contribute to quadriceps tendinopathy as well. As noted, the quadriceps muscle is a collection of 4 very large, powerful muscles starting in the thigh. They move down the leg transitioning to the quad tendon above the knee cap, and then move over the kneecap until forming the patellar tendon that inserts onto the upper shin bone. For more information check out research papers here, here, and here.
The force of gymnastics impact can be anywhere between 15x-18x bodyweight, which is massive. Gymnasts also land 1000s of times per month between training and competition. Along with this, gymnastics culture still struggles with teaching proper landing patterns. Many gymnasts still land in what is known in the research. as a”quad dominant” way, which places more stress on the knee joint instead of spreading the force out across the entire leg/core.
It is this mixture of high force, high repetition, and less than ideal landing patterns that oftentimes causes notable stress to go through the quad and patellar tendon. Even. with the use of soft surfaces, many gymnasts still may have a ton of tendon pain when they run, jump, land, or do squatting-based strength work. While there is evidence that patellar tendon straps may help modify pain, as mentioned in the growth plate section this is not a worthwhile long-term strategy.
Tendinopathies come down to a mismatch between tendon load and tendon capacity. If the tendon does not possess the capacity to handle high forces, or if the tendon does not get enough recovery between high force loading periods, problems may arise. The tendon structure might start to change into less healthy tissue, or tendon breakdown may start to occur, creating pain and a loss of strength/power.
To assist with tendinopathies, a combination of workload modification, strength, and conditioning, and the patient must be used. First, the tendon must be unloaded by reducing high force skills, using softer surfaces, and trying to not do too aggressively of plyometrics. Second, specific strength exercises (typically some version of squatting, lunging, and step-ups) must be used to load the tendon and help rebuild its tolerance. Lastly, time intervals between loading bouts are crucial to help allow the tendon to heal, adapt, and grow stronger. In the long term, time intervals for recovery must be long enough to continuously expose the tendon to higher and higher amounts of force. This is done through more advanced strength work, then power work, then plyometrics.
Once this cycle has been brought the tendon back up to a high level of tolerance, a progressive return to gymnastics specific impact program can be used over 2-4 weeks. I usually recommend soft surfaces, basic skills, and low repetition counts be done 3x/week for 1-2 weeks. Then things can move to harder surfaces, more advanced skills, and higher repetition counts.
Distal Hamstring Tendinopathy
The same general principles of patellar/quad tendinopathy apply to distal hamstring tendinopathy. But, given the very different role of the hamstrings compared to the quads, I give very different activity modification, exercise, and return to sort advice for gymnasts with hamstring issues. First, the hamstrings are much more involved with the “slow down’ eccentric phase. of running or sprinting. Also, the hamstrings are much more stressed during splits, dance jumps/leaps, and bar movements. For these reasons, I have people modify these skills first instead of impact like I do with quad or patellar tendon issues. For some great papers, check out here and here.

In terms of strength progressions, I personally find that starting with more “hip dominant” hinging exercises can load the distal hamstring tendons well without causing too much pain. The progression I use double leg glute bridges, to single-leg glute bridges, to elevated single leg glute bridges, to weighted single leg glute bridges. Then, I try to progress to a combination of kettlebell deadlifts (focusing on load) and physioball curl ins (focusing on a range of motion). These both can progressed from double-leg versions, to single leg versions, like kickstand Romanian deadlifts and single-leg physioball hamstring curl ins. Lastly, the most advanced exercises I use with gymnasts are nordic hamstring lowers, and eccentric split sliders. These tend to be really hard and set the stage for more advanced power/plyo work.
Prior to getting back into gymnastics, I find it’s really important to do gymnastics-specific speed and power work. If this step is skipped, many gymnasts struggle with reinjury when trying to get back to skills. To help, I have athletes do 1-2 weeks of active flexibility work like theraband kicks, tumbl trak jumps/leaps, and drills or basics on each event. I will also give them a progressive sprinting/speed program over 1-2 weeks to rebuild high-intensity running capacity for the vault and floor. Once these seem. tobe going well, I will follow a similar return to gymnastics program as noted above in the patellar/quad tendinopathy section.
Bone Bruises, Stress Fractures, & Fractures
The next category of injuries to tackle is what is broadly known as “bone stress injuries”. I tend to put bone bruises, stress fractures, and acute fractures all into this category even though they have some differences in contributing factors. For one, they are all really just on the same continuum of impact-based overload. Two, they all can be caused by either a one-time high force event (even if accidental) or repetitive overuse.
This being said, it’s worth noting that stress fractures oftentimes have other contributing factors compared to bone bruises/fractures that should always. be investigated. If a gymnast continues to struggle with a single stress fracture that is not healing or has multiple stress fractures in a short period of time, nutrition and proper fueling strategies should be considered. It is very common, particularly in young female gymnasts, for issues like under-fueling or Relative Energy Deficiency in Sport (RED-S) to compromise bone mineral density. When this is paired with high training loads and high impact forces, stress fractures may occur. In these situations, working with physicians and licensed nutritionists is key to recovery
Tibial Plateau Bone Stress Injuries
The first area that can experience a bone stress injury is the top of the shin bone, known as the tibial plateau. While the large femoral condyles, meniscus, and leg musculature can help as massive shock absorbers, the reality is that overload can still occur. In situations of repetitive overload, the top surfaces of the shin bone can first develop a bone bruise with landing forces. If this continues without adequate rest/recovery, it can develop into a hairline stress fracture. Then, if things continue to progress more it can result in a full tibia fracture. As noted in the ankle blog, this can also occur lower in the knee bone with shin splints.

Gymnastics unfortunately always comes with risks. Even with the best, and most robust training programs, accidents can still happen. During freak landings or awkward impacts, the forces can cause sudden bone breaks to occur. In the tibial plateau, this tends to happen with ‘lock-legged’ landings. The front of the femur and the front of the tibial plateau can forcefully hit each other during impact. If this is mild, it may just be a bone bruise. If this is more severe, it can create a full fracture.
There are far too many different types of fractures to cover in this blog post. That said, they may sometimes be able to heal on their own with casting/immobilization. Other times, due to the way the fracture causes the bones to move, plates or rods may be needed to realign things for proper healing. This requires surgical intervention and is obviously more involved. Regardless, bones typically 6-8 weeks to heal, and then an extensive rehab program follows that.
Femoral Condyle Bone Stress Injuries
These are bone bruises that occur on the other side of the knee joint. Instead of the pressure going through the bottom of the knee, it goes through the top of the knee joint. This may be due to the way a gymnast lands, the skills/events they train, their strength profile, or more. In younger gymnasts, the bone or cartilage (more below) may be what gets injured. In older gymnasts, it tends to be the cartilage overlaying the femur that takes all the force. This may create cartilage breakdown like OCD. Regardless of how the femur gets damaged, and whether it is a bone bruise, stress fracture, or acute fracture, the healing principles above in the tibial plateau section are very similar.
One particular bone bruises worth noting is a lateral femoral condyle bone bruise during ACL tears. Due to the extremely violent nature of an ACL tear, as the bones twist the outside knee bone almost always hits the inside lower knee bone. This tends to create a large bone bruise on the femur, which in some studies has been suggested to be one of. the main pain generators. Even 3+ months out, you can sometimes see a notable bone bruise still on MRI. This is something that must be kept in mind, particularly as someone returns back to impact and running during rehabilitation.
Patellar Bone Stress Injuries
Lastly, although rare, there can be issues with the knee cap itself. Repetitive overuse type issues tend to put more stress on the backside of the knee cap, where the cartilage resides. Bone bruises or fractures of the knee cap are more typically caused by accidental falls or trauma directly to the knee cap. Stress fractures may be a progression of inferior pole growth plate inflammation that is not properly rested. This may be seen with falls on beams that create direct contact with the knee. Other times, fractures can be seen when sudden subluxation or discoloration occurs and forcefully causes contact between the knee cap and knee joint. Based on the specific type of fracture, various treatment options like bracing, immobilization, or surgery may be warranted.
Cartilage Injuries & Osteochondritis Dessicans (OCD)
The last major category of injuries to cover is those to the cartilage. As mentioned, the surface of the femur and the surface of the tibia are covered with thick, dense hyaline cartilage to help buffer and disperse impact forces. Due to the presence of the meniscus, it is not as common to hear about cartilage issues on the tibia unless there has been notable meniscus damage or removal. However, the femur bone and the back of the knee cap can develop injuries to the cartilage. If they progress, they can create notable pain, lost motion, and performance issues.
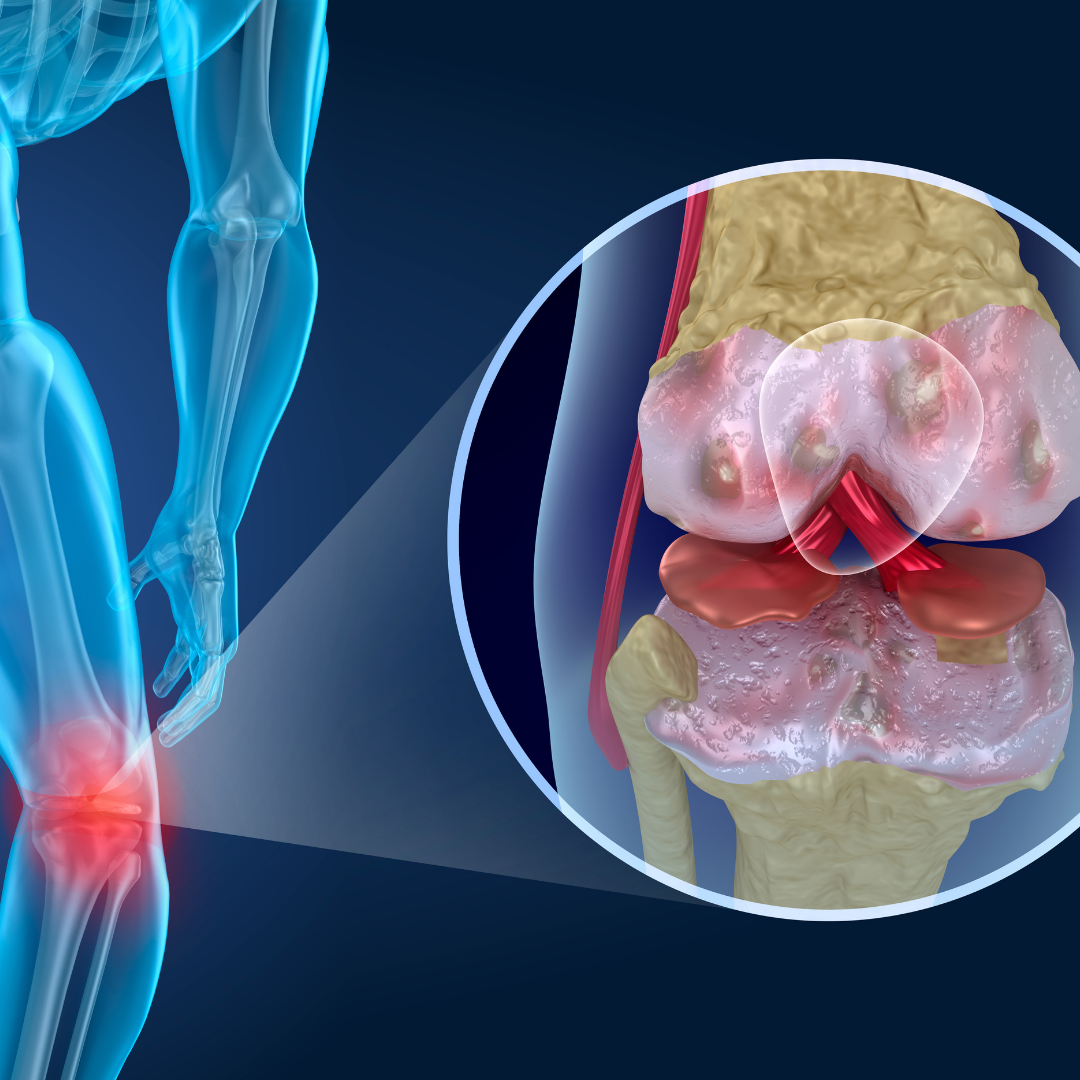
Again, to spare boring people looking for research check out this paper here, here, and here.
As mentioned in the anatomy section, different parts of the cartilage are stressed during knee bending. During the first 30 degrees of knee bending, the bottom portion of the back of the kneecap makes contact with the cartilage of the femur below. With more knee bending down to 70 degrees, progressive increases in contact occur between the back of the knee and the groove of the knee joint it sits in, known as the trochlea. Past 70 degrees of knee bending, progressively more contact is made between these two surfaces and the sport force is spread out further.
During running, jumping, and landings, if the same spot on the back of the knee cap or knee joint groove gets hits over and over again, problems may occur. The progressive damage of cartilage is referred to as OCD or osteochondritis dessicans. Initially, it may just create bruising and inflammation. This is Grade I OCD. As things progress further, the cartilage may start to become starved of blood flow and get even more damage, creating a small divot. This is Grade II OCD. Gymnasts often complain of soreness, stiffness, swelling, and pain. If caught early, a period of rest away from impact and strength work can help someone recover. This is more true of Grade I than Grade II.
If the area continues to take impact without proper rest being given, the deep bone can be cracked creating damage and pieces of bone may break off creating catching, clicking, and pain. This is grade III OCD. Lastly, at its worst, the cartilage is damaged all the way down to the subchondral bone and larger bone fragment pieces are broken off in the joint.
Unfortunately, due to the extensiveness of the damage surgery is almost always warranted. The first surgical line of treatment is usually debridement or causing intentional bleeding to the bone through what is called microfracture surgery. While there may be some positive outcomes with this in lesser grade OCD lesions, in larger or more advanced lesions this may not be the case. To manage Grade III or IV lesions often times a bone plug with undamaged cartilage must be taken from another non-weight-bearing portion of the knee and used to fill in the OCD hole. This is known as an OATS procedure, which stands for osteoarticular transfer system. These surgeries require quite a bit more time, rehabilitation, and a slow return to gymnastics.
How Long Do Knee Injuries Take To Heal?
Respecting The Body’s Healing Process
The question that I get from gymnasts most when treating them for knee injuries is – “when can I go back to gymnastics?” I completely understand athletes wanting to get back to training as fast as possible. It was the same for me as an athlete, and the coaching side of me certainly knows the challenge of having an athlete at practice hung up by these injuries yet wanting to make progress.
That said, we can not magically speed up basic human biology. There are certain things we can do to accelerate, assist, and enhance the natural healing process. But at the end of the day, we have to understand and respect the body’s healing timelines. There is a base timeline for various tissues of the body, and when looking at the literature a realistic timeline for various degrees of injuries. Unfortunately, these don’t change even if we are in the middle of competition season or ahead of a very exciting opportunity.

https://www.physio-pedia.com/File:Wound_healing_phases.png
In almost all cases, taking the time to allow full healing and rehabilitation is the better choice. I’ve been fortunate to work with a few of the world’s best elite and Olympic-level gymnasts/coaches, and I can tell you that the situations where someone has to ‘push through’ for their ultimate goal are few and far between. They occur, but very very rarely. Not to mention, these decisions are often made by adults, their parents, and their medical providers as a team. With this in mind, let’s review some timelines for these various injuries.
Timeframes and Variability for Knee Injuries
We must keep in mind that while there is great science on the healing timelines for many common ankle and foot injuries, there is still a huge variability that can occur. In the big picture, factors like age, genetics, skill level, genetics, past injury history, and more all play a role. Also, the severity and reoccurrence of the injury will make a huge difference in the overall healing timeline.
Oftentimes I will hear people compare one gymnast’s injury to another. Saying that “X” knee injury took 4 weeks in one person, so a sort of similar “Y” injury in another person will be the same. I strongly recommend people do not do this. Even with what seems like the exact same injury, say an inversion ankle sprain, due to many factors mentioned above and more the full return to gymnastics this could be wildly different.
A grade I MCL sprain in a 12-year-old level 7 gymnast who is a bar specialist might take 4 weeks to front handspring vaults, while the same type of grade I MCL sprain in a 15-year-old level 10 gymnast who is a floor/vault specialist may take 8 weeks to get back to Yurchenko layouts. We are also seeing timelines change for common injuries, like ACL tears. It used to be thought, someone. can automatically jog at 3 months, and return to sports at 6 months. But, we are seeing that even for ‘simple’ situations where it is only the ACL repaired, to fully mitigate risk and really prepare someone for high impact sports it may be between 9-12 months.

My best advice is to follow the science of healing timelines (and physician/surgeons protocols when appropriate) but use the major milestones of healing as a guide. These include swelling removal, mitigation of pain, restoration of mobility, a return to daily activities, return of full strength/power, and the ability to tolerate all advanced plyometric skills. I also always teach people early in the rehab process that during the middle of a rehab, when their pain may be gone, they will want to go back to sports but we have to resist the urge. Building strength, power, and capacity take multiple months and lots of work.
A useful rule of thumb to use with people is that for however long a gymnast is out of practice with their injury, it will take 2-3 times as long to return. So say someone has a mild knee sprain that keeps them out for 2 weeks, it will likely take them 4-6 weeks more to fully return. If someone has surgery that keeps them out for 2 months, it will likely take 4-6 months to get back fully.
This being said, in my experience and based on the scientific literature, with less severe injuries like muscular strains, grade 1 sprains, and mild flare-ups of tendonitis, it could be very benign and only take 2-4 weeks to recover.
As the severity of the injury progresses, the timelines extend. Higher degree muscular strains, Grade 2 sprains, mild bone bruises, stress reactions, or more involved tendinopathies, the timeline may extend into the 4-8 week range.
Lastly, the most severe injuries occur like partial/full muscle tears, Grade 3 ligament sprains (aka tears), OCD surgeries, Achilles tendon rupture repairs, and bone fractures take substantially longer likely in the 3-6+ month range and possibly up to a year.
The 4 Phases of Rehabilitation & Goal Milestones For Recovery
When I lecture, do consulting work, or provide rehabilitation for gymnasts, I always try to outline these 4 phases general of rehabilitation. Regardless of the injury, all athletes progress through them. Some injuries move fast if they are less severe, and some move much slower if they are more severe.
Keep in mind that for me, recovery refers to fully getting back to gymnastics without physical or mental hesitancy. Being ‘cleared’ by a medical doctor from a tissue healing point of view doesn’t necessarily mean being fully ready to return to full gymnastics practice. I know and work with many amazing gymnastics-based medical providers, but I know not everyone has this luxury. This is why I try to abide by the 4 Phases of Rehabilitation. They are as follows,
1. The Acute/Subacute Phase – “Put The Fire Out”
Workload Reduction
This is always the hardest thing for gymnasts, parents, and coaches to wrap their heads around, but it takes time for knee injuries to stabilize and calm down. So many people come to the clinic and say “well it’s just a knee, she can do bars and all her strength”. While in some cases, like with mild muscle strains minor irritation, for many other knee injuries this may not be the case. Simply walking, bending the knee, activating the muscles to straighten it all the way, and fast motions may still cause pain. Not to mention, if someone steps. on a mat weird, or comes down off equipment awkwardly like always happens in gymnastics. I am all for gymnasts with knee injuries continuing to find all the things they can do, and make the best use of the downtime, but within reason.
I may definitely give a gymnast an in-depth core, upper body, and non-knee-based cardio program (seated rope slams and biking with arms/one leg). But I really want to educate gymnasts that in the first 2-6 weeks of most knee injuries, it’s going to be about reducing the weight-bearing or impact workload, as well as possibly regular use of the knee outside of the range of motion/strength rehab exercises. We want to focus on getting any swelling down, getting the basic range of motion back, and getting the knee to be less painful while working on strength.
Swelling/Pain Management
It’s crucial that swelling reduction be one of the top priorities with knee injuries. As studies have shown, even small amounts of fluid in the knee joint can be enough to reduce the muscle activity of the quadriceps. Swelling in the knee joint, and around the joint capsule, is also one of the more common reasons for stiffness, reduced range of motion, and soreness during motion.
I always take circumferential measurements at 5cm below the joint line, the joint line, 5cm above the joint line, 10cm above the joint line, and 20 cm above the joint line. The first 3 around the joint line are more for knee swelling, whereas the 10/20cm measurements are more for quad girth changes. I measure these weekly from the start of injury.
So, I am educating gymnasts to use compression sleeves or ace wraps, try to spend a lot of time with their leg elevated above their heart to allow gravity to help, and do as much active motion for their ankles/hips as possible to maintain circulation. If they are cleared for knee motion, I also have them do multiple sets of knee bending/straightening to their tolerance throughout the day. These things, along with hands-on work or anti-inflammatory medication when prescribed, are keys to the early phases of knee rehab.
Restore Basic Flexibility and Range of Motion
Once the swelling is being dealt with, the next most important thing is to try and regain the knee’s full range of motion. In order to do this, both joint mobility and soft tissue flexibility must be worked on.
For joint mobility, the majority of the focus should be on the knee cap moving on the lower knee bones (the patellofemoral joint). When the knee joint bends, the kneecap moves downward on the ‘train tracks’ of the bones underneath it. When the knee joint extends, the knee cap moves upward on the “train tracks” of the bones underneath. So, if there is swelling or stiffness within the tissues around the kneecap, it might be very hard to get the knee to move.
I usually do a lot of hands-on patellar mobilizations up, down, and side to side to help with this. I will teach them to gymnasts if they can safely do them, but keep in mind this is something that must have medical knowledge for. Certain knee injuries, like patellar instability, require a ton of caution with knee cap mobilizations. If done incorrectly or without medical guidance, certain glides (lateral glides in this case) can create further instability or damage to structures like the MPFL may occur.

The knee joint itself (tibiofemoral joint) typically is not the target of too many joint mobilizations in younger, hypermobile gymnasts. This is particularly true if they have intraarticular pathologies like ligament damage, meniscus tears, or cartilage issues. In rare cases, however, someone may need tibial glides to assist in the small amount of rotation that occurs in the knee during the end ranges of bending or straightening. Or, if someone has a very stiff knee after an injury or surgery, some light tibiofemoral glides may be helpful to help the joint move more slowly. These are typically only used in rare cases, however, so they must be under expert medical care.
Outside of the knee joint, the various muscles around the knee joint can very commonly become stiff with the presence of pain, stiffness, a lack of motion occurring, and possibly not putting weight on the knee/being in a brace. In these situations, it is very important that hands-on soft tissue work, manual passive range of motion, and home programs. be used to help restore this mobility. I personally tend to use a combination of heat to warm the tissue up, hands-on massage, IASTM tool work, and light cupping to help facilitate blood flow to the area and a reduction in muscle tone as well as guards to do this. I find this reduces a gymnast’s soreness levels and allows for relaxation that can then help improve the comfort with bending or straightening.
It’s important to note that in almost all knee surgeries, a particular focus must be paid to restoring knee straightening early. While some injuries like anterior meniscal tears or cartilage issues might require caution here, in many other injuries like ACL tears it is an absolute must to get full knee extension/hyperextension back. I have learned from my mentors Mike Reinold and Lenny Macrina, that the most comfortable and effective way to do this is with the heel propped up on a small lift, a moist heat pack on the person’s knee, and lightweight above the knee joint, for 5-10 minutes throughout the day. It is much less anxiety-provoking for the person than things like prone hangs, which typically just create hamstring guarding.
As for knee bending, I have also learned from those same mentors that passive knee bending is likely best done over the edge of a table with a small towel roll under their knee, not with the person lying down. Again, this typically is more comfortable and less anxiety-provoking for the person. In some surgeries, like MCL or patellar instability, doctors may not want the person’s knee to bend past 90 degrees for up to 4-6 weeks. In other injuries like cartilage issues, this may also be true based on the location of the damaged tissue. This is done to protect the healing tissue from taking too much stress in the initial 2-6 weeks. That said, a slow, gradual progression of knee bending is best. Between PT sessions and at-home exercises, I preach a “consistency over intensity” mindset to reduce the risk of the knee getting sore and ‘cranky’ if we push bending motion too fast too soon. Depending on the injury, I’m usually looking to see full heel to buttock knee bending by 6-8 weeks, pending the doctor, I’m working with doesn’t have limitations put in place like mentioned above.
Maintain/Restore Basic Strength
One of the most important aspects of knee rehabilitation is strength. As research in many different injuries like patellofemoral joint pain, patellar tendinopathy, ACL tears, meniscus tears, & more have shown – proper loading through exercise and strength programs is essential.
In the early phases of knee rehabilitation, this can be very hard to do as someone often times has pain that may limit their loading tolerance. This is where. itis crucial to understand not only what is a normal response to exercise vs an abnormal response that increases symptoms. For most cases (minus some surgeries) I tell people that some sort of discomfort is expected, say a 2-3/10, as long as the pain levels do not increase after exercise or elevate in the day following exercise. Muscular soreness and general fatigue are expected, where sharper or more intense pain is not. I also closely monitor swelling levels of the knee joint, and range of motion, during this time. If exercise causes the knee to increase in swelling or create losses in the range of motion, we may be pushing too fast too soon.
We also must remember that certain exercises may stress different parts of the knee more or less depending on the injury. Doing forward lunges versus backward lunges, squats versus hip lifts, and Nordic hamstring lowers versus RDLs all may have very different impacts on the tissues of the knee joint. Someone working with a gymnast must have a good grasp of the injury, the exercises that will stress that tissue to regain strength and the principles of progressive overload to help logically progress over time.
This being said, usually in the very early stages of rehab, I am looking to do table-based exercises that are more ‘open chain’ in nature. Things like quad sets, straight leg raises with ankle weights, knee extensions, hamstring curls, and banded hip work. I’m also trying to load the hips and calves as much as I can. I am always using NMES to help facilitate the quad muscle, and Blood Flow Restriction training to try and get more of a strength training effect when we can’t load very much.
While some people knock these exercises, I think they have a time and a place in the early stages of rehab and particularly surgery. We don’t want to get stuck on them forever, but they set the stage for later work.
As soon as someone is able, ready, has clearance from their doctor, I am trying to progress to things like hip bridges, mini squats, step-ups, step downs, cone stepping, and partial range of motion split squats. I continue to maintain the basic direct quad/hamstring loading above, but usually, I’m starting to build a more holistic program. This helps set things up for the next Phase.
It is also crucial to regain strength, in particular the quad, to assist if someone has been using crutches, a brace, or has limited weight-bearing ability.
Return To Normal Walking
The last big goal of this acute phase is to normalize walking. For some injuries, this happens in days and does not require much progression. For other more severe injuries or surgeries, the use of a walking boot, crutches, or other weight-bearing precautions makes this occur over multiple weeks. This progression back to normal weight-bearing is important not only for mobility and strength but also because the active muscle pumping action of the lower body helps to promote blood flow in and out of the area.
When cleared, and per the guidance of medical doctors, I try to recommend that a slow weaning process occurs for weight-bearing. This helps prevent the sudden irritation of foot muscles/tendons of the injured area. To do this, I generally teach athletes to progress over the course of a week. So say they are on two crutches, we might spend start with just a few hours in the morning using one crutch but two for the rest of the day.
Then, over the week we may add 2-3 more. hours of morning one crutch time, and less afternoon two crutch time. By the end of the week, they can try a full day on one crutch. Then we do the same from one crutch to no crutches. I do a similar progression for weaning out of a boot or immobilizer if that was used.
Once the athlete has less pain, minimal swelling, good progress in flexibility returning, returning strength levels, and relatively normal walking tolerance, we progress to phase 2.
2. The Intermediate Phase – “Be A Human Again”
In this phase, generally from the 4-8 week range, the focus is very much so on strength and conditioning. The main goals are that someone can tolerate all the non gymnastics things they have to do in their day-to-day life. Climb stairs, walk all day, get to classes, lift things, and so on.
In order to do this, we must continue to really make strength and exercise progressions the main focus of the program. While I will continue to do some hands-on work for a range of motion and mobility, the majority of my time is spent on building a more robust exercise program. This is done through a combination of continued direct knee loading, compound movement patterns, balance work, and rebuilding capacity.

The compound movements that I am looking to get back to are squatting, hinging, split pelvis positions, and single leg work. I usually aim for goblet box squats for squatting, weighted hip lifts/kettlebell deadlifting for hinging, split squats for split pelvis patterns, and step-ups/step downs for single leg work.
I also can’t stress enough how important working other areas of the kinetic chain are. As research has shown, the calf is crucial for impact force absorption and protecting the knee. While the value core/hip strength directly on knee pain is debated, the hips are vital in producing power in absorbing force in all sports so we need to keep pushing that. They are also crucial for trying to maintain sound biomechanical positions during sports. This said, things like seated/standing calf raises, planking, anti-rotation pressing, sled push/pulls, suitcase/farmer carries, side plank clamshells and resisted band walking work are always in my programs.
Of note, during this phase, it may also be useful for an athlete to count their steps over the course of the day. As they return back to full activity, being on their feet for the entire day/week may add up and create some soreness. Tracking steps can help to slowly increase the total workload being done.
3. The Advanced Phase – “Be An Athlete Again”
In this phase which is commonly missed or not really focused on, we are aiming to restore the basic qualities that all athletes need. Which is along with the movements above, the ability to run, jump, land, change direction, and be powerful. This sets the foundation for a smooth return to gymnastics in the next phase. Without it, it is very easy for gymnasts to not develop their full capacity and struggle with reinjury once they try to start skill work. I find that many people tend to not do this phase because oftentimes gymnasts have no pain, and feel ready to go. Take it from me though, it is worth the time and effort to go slow here and respect normal adaptation timelines. I generally find this phase occurs between the 12-16/20 week timeframes, again based on the injury severity.

First comes the need to start reintroducing plyometrics and impact work. This is often an intimidating area for gymnasts and medical providers, but if the first few phases are done well, there is typically no issue with starting to do impact work. Keep in mind for some injuries like cartilage damage or fractures, this will take a while and will require clearance from a doctor/surgeon. These are the exercises I use to start this
- 20 Pogo hops
- 20 In and out hops
- 20 Scissor hops
- 2 laps Jogging laps forwards and backwards
- 2 laps Skipping laps forward and sideways
- 2 laps Carioca and side shufle laps
- Vertical force – seated dumbbell jumps, box jumps, high skips, depth drops, medball slams and throws
- Horizontal force – broad jumps, forward sprinting/running progressions, and change of direction drills
These tend to be a bit more demanding, so usually I program them in sets of 2-4 repetitions of 3-5. As with the phase above, these can be built into programs and slowly progress over time until gymnasts are tolerating high power and high impact-based drills.
I also like progressing some. of the dynamic stability work. This can include unstable surface squatting/balance work, or more jumping and landing progressions. to one leg with rotational demands.
4. The Return to Sport Phase – “Be A Gymnast Again”
This is another very important, yet sometimes murky, area of gymnastics rehabilitation. While there has been great work by some researchers suggesting sports progressions, and other work to look at in baseball/tennis/golf, the reality is that gymnastics still largely has a lack of objective science-based return to sport protocols. Based on these tools and others, there are 3 main variables that I use to make return to gymnastics programs.
- Surface – soft surfaces like pit/trampoline, to medium surfaces like rod strips and using 8″ mats, to hard surfaces like spring floors or beams
- Force per skill – low impact force basics and drills, to moderate impact force skill or skill combination work, to high force power tumbling or vaulting or dismounts
- Repetitions – low repetitions per week, to moderate repetitions per week, to high repetitions per week

When I make these programs, I take the skills that a gymnast is currently performing and map them across the week. I have gymnasts do skill work 3 days per week, with 24 hours in between, while maintaining their strength program. I typically progress them every 2 weeks, making sure not to increase the surface demand, force per skill, and repetitions all at once. This typically looks like
- Weeks ½ – Soft Surface, Drills/Basics, Low Repetition volume
- Weeks ¾ – Soft/Medium Surface, Skills, Moderate Repetition volume
- Weeks ⅚ – Medium/hard, Harder skills, Moderate Skill Volume
- Week ⅞ – Hard Surfaces, Hard Skills, no > 7 reps per skill per day
Again, keep in mind that with mild injuries each phase may only take 1 week, totaling 4 weeks. In more severe injuries or those requiring surgeries, it may take 2-4 weeks for each phase, expanding the total time out to possible 8 or 16 weeks. While there are many caveats to these rehab programs, and individualization must always be applied based on the unique case, hopefully, these general guidelines can be useful.
If you want a very in depth break down of returning to impact after an injury, check out this popular YouTube video I made.
What Can Be Done To Speed Up Healing in Gymnastics Knee Injuries?
As I mentioned, we can’t magically eliminate the natural healing timelines of tissues. But, there are many things that we can do to assist in the healing process and help optimize the body. In my experiences, these are typically less talked about as focus points. I feel that far too many people are looking for the “best exercise” or new fads in technology to try and speed up the healing process. This typically just leads to frustrations and stalled progress. Based on the literature I have reviewed and my experiences, the biggest things we can do to assist in injury recovery are
Time
As mentioned, allowing for proper timelines of healing is crucial. We want to make sure that we apply the optimal dose of loading, followed by the optimal dose of recovery, to get tissue adaptation. If we apply too much load too soon or don’t allow enough time for recovery, we can spin our wheels and run into frustrations. As literature supports, we want to shoot for the optimal dose of stress followed by the proper period of rest for the body to heal. While this will vary from tissue to tissue (tendon vs bone vs cartilage), it still applies universally.
Sleep
Getting enough sleep, and getting high-quality sleep, are both enormously important for our body’s recovery. I refer people to some great researchers like Matthew Walker and Andrew Huberman for the great information. Some of the most common tips they suggest are
- Aiming to look at morning sunlight within the first 60 minutes of waking, and trying to see evening sunsetting light
- Having consistent waking/sleeping schedules, even on weekends
- Avoiding screens or blue light 1- 2 hours prior to bed
- Sleeping in a slightly cooler room, 68 degrees F or below
- Avoiding caffeine intake 8-10 hours before bed
- Avoiding food intake 1-2 hours before bed
Proper Fueling
Tissue healing depends on having the proper fuel sources for the body to build that tissue from. It is absolutely crucial that gymnasts are getting not only enough food intake but also high-quality ingredients, for their bodies to heal. This is not my area of expertise, but I’m lucky to be friends with some expert medical providers who specialize in nutrition for gymnasts. For more information, check out Christina Anderson, Josh Eldridge, and Kerry Blair.
Compression & Active Movement To Tolerance
As outlined extensively above, there has been a movement away from icing and into promoting movement and activity to tolerance. For those looking to help speed up the recovery process, we can try to manage the swelling, motion, and blood flow as much as possible.
Static compression garments, like compression sleeves or ace wraps, can be useful. However, intermittent pneumatic compression, say in the form of mechanical dynamic compression garments like Normatec’s, has great support in the literature to restore cellular environments for recovery. While there is not extensive medical literature on ankle injuries and compression, I do try and build it into programs when appropriate.
Proper Exercise Progressions
Above all else, we have to remember that the human body senses, responds, and adapts to the appropriate dosage of load (the geeky term being mechanotransduction). The 4 phases of rehabilitation, and all the exercises I outlined above, provide the framework for how this can be done for gymnasts with ankle and foot injuries. It’s also the reason why strength and conditioning principles are so crucial. We must be using both external weight training and body weight strength training to help increase capacity, and build a robust athlete through physical preparation.
How Do We “Prevent” Knee Injuries in Gymnastics?
So with all this in mind, what can we do to stay ahead of injuries? We do have many great tools we can think apply given all this information, but it is worth noting that ‘preventing’ injuries probably isn’t realistic.
For one, injuries are extremely complex with multiple factors contributing to them. Even the best science-based “prehab’ program can address all of these.
Second, gymnastics (and all sports) are just inherently risky. There will always be bumps, bruises, and accidents that happen. While I’m certainly a fan of trying as much as we can to reduce the risk of injuries, being realistic is also important. I often don’t use the work “prevent” but more “reduce risk”. That said, let’s take a look at some evidence-based concepts that we can apply to reduce the risks of foot and ankle injuries.
Workload Planning, Management, & Monitoring
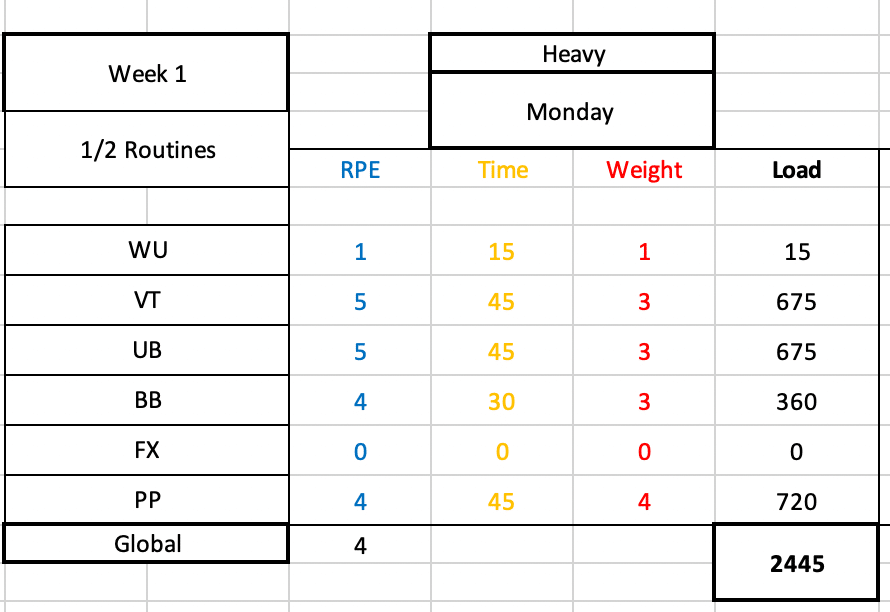
While the workload research is progressing to be less about ‘injury prevention and more about monitoring, there is great data thus far to suggest that keeping a close eye on workload can be useful.
For one, we want to make sure that we don’t subject gymnasts to rapid, unplanned, sudden spikes in impact workload. This rapid increase in load might be too much for a gymnast’s ankle/foot to handle and may contribute to elevated injury risk. This often times happens just before competition season, or when coaches might get over-excited and throw lots of new drills or plyo conditioning at gymnasts.
In another light, we also don’t want to undertrain gymnasts so that they are unprepared for the demands of gymnastics. If gymnasts are not doing an appropriate amount of skill, strength, and impact training, we may set them up for issues. Another theme in the workload research is that hard, but intelligently designed training programs, are helpful to try and reduce injury risk and increase performance.
We find the workload ‘sweet spot’ of not too much but too little, by being meticulous about the science of periodization and planning along with constant communication. We must map out the entire year, month-to-month goals, week-to-week force progressions, and daily assignments, so that we can create a progressive increase in load and back off when needed to allow recovery.
Great Strength & Conditioning Programs

This goes hand in hand with the workload concept, but formal science-based strength programs are one of the best tools that we have in helping reduce injury risk and increase performance. There is a great body of evidence suggesting that strength training, primarily with the proper usage of external weight training, is fantastic for athletes. I’m a huge fan of external weight lifting and bodyweight gymnastics being used together, in what I call ‘hybrid’ strength and conditioning programs. This is of particular importance for the lower body and foot/ankle injuries, given the forces that gymnasts experience.
Despite the overwhelming amount of evidence for the use of weight training, gymnastics culture is still largely resistant to adopting it. Many fear that it will make gymnasts ‘bulky’, lose their flexibility, or get hurt. Again, the research conflicts with this particularly when proper coaching, proper programming, and proper progression is used. For more information on this, check out this popular blog post I wrote.
Fostering Cultural Changes Around Early Specialization, Year-Round Training, and Age Guidelines
Continuing on the challenge of cultural norms, the continued focus on early specialization, year-round training, and very young gymnasts possibly being pushed too hard/too soon are huge concerns.
As with strength and conditioning, there is a massive amount of research highlighting the possible dangers of this. Both year-round training and early specialization have been associated with elevated injury risk, elevated burnout rates, and drops in long-term performance. While I do believe that there will be some lean towards earlier ages for gymnasts, particularly if they have high level goals, the tough reality is that we need to have some serious conversations about if this is beset for gymnasts’ health and long term performance.
I feel this matters most in situations like impact-based ankle/foot injuries. Doing only gymnastics from an early age, and doing it all year long, maybe subject young athletes to massive amounts of high force impact repetitions. This may create a notable risk of various injuries, and also contribute to burnout or stalled long-term performance.
Similar to this, currently are no guidelines for how many training hours per week young gymnasts of various levels should be training. How many hours per week should an 8-year-old level 6 gymnast train? What about a 13-year-old level 10? Is it ideal for the age limit of senior elite gymnastics to be 16, not 18?
I don’t have the answers to these questions. But, if we want to see actual, lasting change on the rates of ankle (and all) injuries, with higher levels of long-term performance, we must get groups of experts from all disciplines to get together and brainstorm these ideas. Particularly those around training hours, and changing our culture to not ask pre-pubertal 10-14-year-old gymnasts to be elite athletes well before they are physically or mentally ready.
Teaching Excellent Gymnastics Technique & Landing Technique
While this is not something with a ton of scientific support, it makes sense to apply the idea that a focus on excellent basics, technical foundations, and mastering proper skill progressions over multiple years is what’s best for gymnasts. During the younger years when growth and puberty are occurring, we want to help protect athletes’ bodies by teaching and using excellent techniques. This means teaching proper running, tumbling, bounding, and dismount techniques. It also means applying the best science to proper landing techniques and making sure that the judges are not deducting when athletes land properly.
This requires gym cultures that are willing and able to invest in these more ‘boring’ sides of the sport. It also requires a culture that as a whole is willing to build an educational model where coaches are required to go through academic and mentorship to learn the best practices here. We can’t just throw a bunch of drills at coaches through online forums or lectures and expect them to go back to their gym and magically know what to do. In my opinion, I think we need a 1 year combined academic/mentorship model for anyone wanting to coach gymnastics. Then, an additional 1 year of advanced course work and mentorship for those who wish to work in the higher levels of optional, college, and elite gymnastics.
Mat Usage and Surface Monitoring
Lastly, one of the major things that we can do to help reduce the risk of ankle and foot injuries in gymnastics is by utilizing the massive amount of matting technology we have at our disposal. Various sting mats, 8″ or 12″ mats, resi pits, and other devices allow gymnasts to not only train high-level skills but also compete with buffered forces. I know that financial barriers are sometimes here, but athlete safety and longevity are by far and away from the number one priority for us.
To go along with this, we must meticulously plan the progression over the competitive year from soft to semi-firm, to hard surfaces. If people think about starting to compete in December of a year, we must look backward 3 months in advance and design slow, methodical progressions from softer to harder surfaces. As we’ve seen, jumping too fast into hard surfaces without adequate time and physical preparation will significantly increase the possible injury risk. Again, education is huge here for coaches, medical providers, strength coaches, and sports scientists to all come together and create consensus statements that will help the community.
What Do We Do If Gymnast’s Knee Injuries Aren’t Improving?
I would be denying the obvious if I didn’t admit that despite all the best practices, there are times when gymnasts’ ankle and foot injuries simply do not make progress. They take the appropriate time off, move through rehabilitation, and try to regain strength, but whenever they try to do their skills pain returns. In my experiences, here are the biggest factors to look into if someone can’t seem to get over their foot or ankle injury.
Culture Issues
This is by far and away from the biggest ‘elephant in the room’ issue that comes up when I work with gymnasts who seem to have long-lasting foot and ankle injuries. It’s crucial to make sure that the gym and community culture is not only supportive but aligned. By aligned, I mean sharing common goals.
In my experience, I find that sometimes the goals of the gymnast have changed for them to no longer want to train in a particular level of the sport, or honestly, they may not want to do gymnastics anymore. If open communication is not used, and a gymnast’s goals are not shared with parents, coaches, and medical providers, friction will result. An honest discussion about this is the first place to start if someone is struggling to get back.
Although it is less common these days, the brutal reality is that in some gyms a toxic culture exists where there is a lack of trust and athlete-centered focus. If adults are being a bit too selfish, and are not respecting someone’s injury or medical advice, they may downplay or disregard the athlete’s pain levels.
Or they may try to ‘test the waters’ on skills and go back to impact work too fast. Or, they may not be open to modifying skill profiles of gymnasts (say a less hard dismount/tumbling pass in an upcoming meet, or only doing 2 events). In some situations, gyms may not be willing to go way back to basics and correct skill techniques or get stronger as they are in season and want to rush back to competing.
When this is happening, my first recommendation is always to have a private discussion with everyone involved through the lens of empathy. Everyone likely wants the same things – for athletes, coaches, and parents to be happy and healthy. When professional discussion can occur, you can talk about the issues head-on, brainstorm solutions, and take action to change things.
If you are part of a place where someone is not open to communication or is unwilling to change, you have to ask yourself “Is this a good fit?”. Sometimes hard choices have to be made about parents, coaches, or gyms. It can be challenging, but nothing is worth sacrificing someone’s term mental or physical health.
Rehabilitation is Not Challenging Enough
Just as there can be issues with the sport and coaching side of things, there can be issues with the medical side of the fence as well. Most often, issues related to not applying the science of strength and conditioning to rehabilitation.
I find in many programs, the basic exercises that are very appropriate in the first two phases of rehabilitation never progress to advanced strength, plyometric, or power exercises. This can leave athletes short, as they are not able to rebuild their capacity. Then, once they try to go back to even basic gymnastics skills, the pain returns. Sometimes taking a step back, and really hammering strength for 4-6 weeks, is the key to getting over the hump.
In other situations, medical professionals may really lack an understanding of the sport of gymnastics. If they do not understand skill names, events, levels, and different training equipment that can be used, it might be easy to get lost. It is challenging to find medical providers who understand gymnastics, I admit this. But, thanks to the internet and many online forums, there are certainly places to develop and share this knowledge. There are also many educational platforms that can aid people in helping gymnasts more specifically.
Return To Sport Progression is Too Fast
I commonly find that the return to sports progression is too fast following ankle or foot injuries. This could be due to gymnasts not feeling pain, meet season pressure, a lack of guidance, external pressure, but the reality is that if we go too fast too soon it is very easy to flare issues up.
We have to remember that once we add in more skills or training days, we are likely adding hundreds and hundreds of impacts per week. These impacts are very high force, even when basics or soft surfaces are used. In some cases with higher levels, I find that even progressing every 2 weeks for 8 weeks might be too much. We must always respect the natural adaptation process, and be understanding when someone may hit a speed bump needing to pump the breaks a bit.
Skill Technique Not Being Corrected
This is typically more on the gymnast, but it’s crucial that skill technique and landing technique be corrected if it’s an issue. Athletes who struggle with shaping positions, basic strength, tumbling mechanics, or skill foundations may have a tough time with getting back to high-impact skills. This is typically the most common for floor, vault, and dismounts.
Following injury, the ankle and feet will. be more sensitive to short landings or high forces. If someone is throwing their head out on a floor tumbling pass causing them to land short or doesn’t understand tapping mechanics to fully rotate a dismount around, this must be corrected. Without this, problems may continue to surface over and over.
Lacking Patience with Growth and Development
This last one is really more about the entire sport of gymnastics changing their perspective on the expectations we place on children in the sport. Up until the age of 16 (or more), it is a constant uphill battle against growth and development. This is a normal part of being a human that is out of the gymnast’s control. They will grow, lose flexibility temporarily, lose strength, struggle with skills, have hormonal/mental health issues, and much more.
Gymnasts are already so hard on themselves, and if an adult is lacking compassion or is putting more pressure on them, it’s a nightmare. I see this often when a young gymnast is being asked to return back quickly after an ankle/foot injury, saying they will “miss their shot” if they don’t do _______ competition. This is a really dangerous approach to take, and has to be pushed out of our sport.
Concluding Thoughts
So that brings this absolutely monstrous, epic blog post to a close. While I highly doubt that anyone read the entire thing, my hope is that you were able to jump around to get the relevant pieces of information they needed. I will continue to update this blog post over the years as I learn more, new science emerges, and I gain more experience. As mentioned above, if you want more on the topic you can check out SHIFT’s Gymnastics Strength and Conditioning Course, our monthly membership group The Hero Lab, or our full CEU approved Gymnastics Lower Extremity course for medical providers.
![]()
If there are other issues not covered here, or things you would like to learn more about, be sure to reach out to us on social media so I can put it on my to do list!
Take care,
Dave
Dr. Dave Tilley DPT, SCS
CEO/Founder of SHIFT Movement Science
References
- Kerr ZY, Hayden R, Barr M, Klossner DA, Dompier TP. Epidemiology of National Collegiate Athletic Association Women’s Gymnastics Injuries, 2009-2010 Through 2013-2014. J Athl Train. 2015 Aug;50(8):870-8. doi: 10.4085/1062-6050-50.7.02. Epub 2015 Jul 21. PMID: 26196702; PMCID: PMC4629945.
- MOON Knee Group, Spindler KP, Huston LJ, Chagin KM, Kattan MW, Reinke EK, Amendola A, Andrish JT, Brophy RH, Cox CL, Dunn WR, Flanigan DC, Jones MH, Kaeding CC, Magnussen RA, Marx RG, Matava MJ, McCarty EC, Parker RD, Pedroza AD, Vidal AF, Wolcott ML, Wolf BR, Wright RW. Ten-Year Outcomes and Risk Factors After Anterior Cruciate Ligament Reconstruction: A MOON Longitudinal Prospective Cohort Study. Am J Sports Med. 2018 Mar;46(4):815-825. doi: 10.1177/0363546517749850. PMID: 29543512; PMCID: PMC6036619.
- Katz N.B., et al. Lower Extremity Injuries in Gymnastics. In Gymnastics Medicine. 209-231. 2020. Springer-Nature. Switzerland.
- O’Kane JW, Levy MR, Pietila KE, Caine DJ, Schiff MA. Survey of injuries in Seattle area levels 4 to 10 female club gymnasts. Clin J Sport Med. 2011 Nov;21(6):486-92. doi: 10.1097/JSM.0b013e31822e89a8. PMID: 21959798
- Westermann RW, Giblin M, Vaske A, Grosso K, Wolf BR. Evaluation of Men’s and Women’s Gymnastics Injuries: A 10-Year Observational Study. Sports Health. 2015 Mar;7(2):161-5. doi: 10.1177/1941738114559705. PMID: 25984262; PMCID: PMC4332645
- Kolt GS, Kirkby RJ. Epidemiology of injury in elite and subelite female gymnasts: a comparison of retrospective and prospective findings. Br J Sports Med. 1999;33(5):312-318. doi:10.1136/bjsm.33.5.312
- Wadley GH, Albright JP. Women’s intercollegiate gymnastics. Injury patterns and “permanent” medical disability. Am J Sports Med. 1993 Mar-Apr;21(2):314-20. doi: 10.1177/036354659302100224. PMID: 8465930.
- Wadley GH, Albright JP. Women’s intercollegiate gymnastics. Injury patterns and “permanent” medical disability. Am J Sports Med. 1993 Mar-Apr;21(2):314-20. doi: 10.1177/036354659302100224. PMID: 8465930.
- Sweeney, E. (Eds). Gymnastics Medicine. 202. Springer-Nature. Switzerland.
- Sands WA. Characteristics of Gymnastics Injuries. In Jemni The Science of Gymnastics: Advanced Concepts 2018. Routledge
- Bruggemann GP., Hume PA. Biomechanics related to injury. In Handbook of Sports Medicine: Gymnastics. 2013. Wiley-Blackwell
- Atikovic A. Kalinski SD., Cuk I. Age trends in artistic gymnastics across world championships and the Oylmpic Games from 2003 o 2016. Science of Gymnastics Journal 9(3):251-263
- Balyi I. Long-Term Athlete Development: Trainability in Childhood and Adolescence Windows of Opportunity, Optimal Trainability. Victoria: National Coaching Institute British Colombia & Advanced Training and Performance Ltd. 2004. Found at – https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.732.4200&rep=rep1&type=pdf
- Balyi I., Way R., Higgs C. Long Term Athletic Development. 2103. Human Kinetics. Champaign, IL, USA.
- Lauersen JB, Bertelsen DM, Andersen LB. The effectiveness of exercise interventions to prevent sports injuries: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med. 2014 Jun;48(11):871-7. doi: 10.1136/bjsports-2013-092538. Epub 2013 Oct 7. PMID: 24100287.
- Webster KE, Hewett TE. Meta-analysis of meta-analyses of anterior cruciate ligament injury reduction training programs. J Orthop Res. 2018 Oct;36(10):2696-2708. doi: 10.1002/jor.24043. Epub 2018 Jun 13. PMID: 29737024.
- Lloyd RS, Faigenbaum AD, Stone MH, Oliver JL, Jeffreys I, Moody JA, Brewer C, Pierce KC, McCambridge TM, Howard R, Herrington L, Hainline B, Micheli LJ, Jaques R, Kraemer WJ, McBride MG, Best TM, Chu DA, Alvar BA, Myer GD. Position statement on youth resistance training: the 2014 International Consensus. Br J Sports Med. 2014 Apr;48(7):498-505. doi: 10.1136/bjsports-2013-092952. Epub 2013 Sep 20. PMID: 24055781.
- Dahab KS, McCambridge TM. Strength training in children and adolescents: raising the bar for young athletes? Sports Health. 2009 May;1(3):223-6. doi: 10.1177/1941738109334215. PMID: 23015875; PMCID: PMC3445252.
- Zwolski C, Quatman-Yates C, Paterno MV. Resistance Training in Youth: Laying the Foundation for Injury Prevention and Physical Literacy. Sports Health. 2017;9(5):436-443. doi:10.1177/1941738117704153
- Peitz M, Behringer M, Granacher U. A systematic review on the effects of resistance and plyometric training on physical fitness in youth- What do comparative studies tell us? PLoS One. 2018 Oct 10;13(10):e0205525. doi: 10.1371/journal.pone.0205525. Erratum in: PLoS One. 2018 Nov 14;13(11):e0207641. PMID: 30304033; PMCID: PMC6179270.
- Pollard CD, Sigward SM, Powers CM. ACL Injury Prevention Training Results in Modification of Hip and Knee Mechanics During a Drop-Landing Task. Orthop J Sports Med. 2017 Sep 8;5(9):2325967117726267. doi: 10.1177/2325967117726267. PMID: 28959697; PMCID: PMC5593213.
- Bergeron MF, Mountjoy M, Armstrong N, et al International Olympic Committee consensus statement on youth athletic development British Journal of Sports Medicine 2015;49:843-851.
- LaPrade RF, Agel J, Baker J, Brenner JS, Cordasco FA, Côté J, Engebretsen L, Feeley BT, Gould D, Hainline B, Hewett T, Jayanthi N, Kocher MS, Myer GD, Nissen CW, Philippon MJ, Provencher MT. AOSSM Early Sport Specialization Consensus Statement. Orthop J Sports Med. 2016 Apr 28;4(4):2325967116644241. doi: 10.1177/2325967116644241. PMID: 27169132; PMCID: PMC4853833.
- Myer GD, Jayanthi N, Difiori JP, et al. Sport Specialization, Part I: Does Early Sports Specialization Increase Negative Outcomes and Reduce the Opportunity for Success in Young Athletes?. Sports Health. 2015;7(5):437-442. doi:10.1177/1941738115598747
- Myer GD, Jayanthi N, DiFiori JP, et al. Sports Specialization, Part II: Alternative Solutions to Early Sport Specialization in Youth Athletes. Sports Health. 2016;8(1):65-73. doi:10.1177/1941738115614811
- Lloyd RS, Faigenbaum AD, Stone MH, Oliver JL, Jeffreys I, Moody JA, Brewer C, Pierce KC, McCambridge TM, Howard R, Herrington L, Hainline B, Micheli LJ, Jaques R, Kraemer WJ, McBride MG, Best TM, Chu DA, Alvar BA, Myer GD. Position statement on youth resistance training: the 2014 International Consensus. Br J Sports Med. 2014 Apr;48(7):498-505. doi: 10.1136/bjsports-2013-092952. Epub 2013 Sep 20. PMID: 24055781.
- Myers AM, Beam NW, Fakhoury JD. Resistance training for children and adolescents. Transl Pediatr. 2017;6(3):137-143. doi:10.21037/tp.2017.04.01
- Windt J, Gabbett TJ. How do training and competition workloads relate to injury? The workload-injury aetiology model. Br J Sports Med. 2017 Mar;51(5):428-435. doi: 10.1136/bjsports-2016-096040. Epub 2016 Jul 14. PMID: 27418321.
- Windt J, Zumbo BD, Sporer B, MacDonald K, Gabbett TJ. Why do workload spikes cause injuries, and which athletes are at higher risk? Mediators and moderators in workload-injury investigations. Br J Sports Med. 2017 Jul;51(13):993-994. doi: 10.1136/bjsports-2016-097255. Epub 2017 Mar 8. PMID: 28274916.
- DiFiori JP, Benjamin HJ, Brenner JS, Gregory A, Jayanthi N, Landry GL, Luke A. Overuse injuries and burnout in youth sports: a position statement from the American Medical Society for Sports Medicine. Br J Sports Med. 2014 Feb;48(4):287-8. doi: 10.1136/bjsports-2013-093299. PMID: 24463910.
- Ahlquist S, Cash BM, Hame SL. Associations of Early Sport Specialization and High Training Volume With Injury Rates in National Collegiate Athletic Association Division I Athletes. Orthop J Sports Med. 2020;8(3):2325967120906825. Published 2020 Mar 12. doi:10.1177/2325967120906825
- Mosher A, Fraser-Thomas J, Baker J. What Defines Early Specialization: A Systematic Review of Literature. Front Sports Act Living. 2020 Oct 27;2:596229. doi: 10.3389/fspor.2020.596229. PMID: 33345176; PMCID: PMC7739675.
- Sweeney E, Howell DR, Seehusen CN, Tilley D, Casey E. Health outcomes among former female collegiate gymnasts: the influence of sport specialization, concussion, and disordered eating. Phys Sportsmed. 2021 Nov;49(4):438-444. doi: 10.1080/00913847.2020.1850150. Epub 2020 Nov 23. PMID: 33186080.
- Zaremski JL, Zeppieri G Jr, Tripp BL. Sport Specialization and Overuse Injuries in Adolescent Throwing Athletes: A Narrative Review. J Athl Train. 2019;54(10):1030-1039. doi:10.4085/1062-6050-333-18
- Post EG, Rosenthal MD, Pennock AT, Rauh MJ. Prevalence and Consequences of Sport Specialization Among Little League Baseball Players. Sports Health. 2021 May-Jun;13(3):223-229. doi: 10.1177/1941738120970956. Epub 2021 Feb 3. PMID: 33530863; PMCID: PMC8083145.
- Aicale R, Tarantino D, Maffulli N. Overuse injuries in sport: a comprehensive overview. J Orthop Surg Res. 2018;13(1):309. Published 2018 Dec 5. doi:10.1186/s13018-018-1017-5
- Bell DR, Post EG, Biese K, Bay C, Valovich McLeod T. Sport Specialization and Risk of Overuse Injuries: A Systematic Review With Meta-analysis. Pediatrics. 2018 Sep;142(3):e20180657. doi: 10.1542/peds.2018-0657. Epub 2018 Aug 22. PMID: 30135085.
- Evans JW. Periodized Resistance Training for Enhancing Skeletal Muscle Hypertrophy and Strength: A Mini-Review. Front Physiol. 2019 Jan 23;10:13. doi: 10.3389/fphys.2019.00013. PMID: 30728780; PMCID: PMC6351492.
- Lauersen JB, Bertelsen DM, Andersen LB. The effectiveness of exercise interventions to prevent sports injuries: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med. 2014 Jun;48(11):871-7. doi: 10.1136/bjsports-2013-092538. Epub 2013 Oct 7. PMID: 24100287.
- Webster KE, Hewett TE. Meta-analysis of meta-analyses of anterior cruciate ligament injury reduction training programs. J Orthop Res. 2018 Oct;36(10):2696-2708. doi: 10.1002/jor.24043. Epub 2018 Jun 13. PMID: 29737024.
- Lloyd RS, Faigenbaum AD, Stone MH, Oliver JL, Jeffreys I, Moody JA, Brewer C, Pierce KC, McCambridge TM, Howard R, Herrington L, Hainline B, Micheli LJ, Jaques R, Kraemer WJ, McBride MG, Best TM, Chu DA, Alvar BA, Myer GD. Position statement on youth resistance training: the 2014 International Consensus. Br J Sports Med. 2014 Apr;48(7):498-505. doi: 10.1136/bjsports-2013-092952. Epub 2013 Sep 20. PMID: 24055781.
- Dahab KS, McCambridge TM. Strength training in children and adolescents: raising the bar for young athletes? Sports Health. 2009 May;1(3):223-6. doi: 10.1177/1941738109334215. PMID: 23015875; PMCID: PMC3445252.
- Zwolski C, Quatman-Yates C, Paterno MV. Resistance Training in Youth: Laying the Foundation for Injury Prevention and Physical Literacy. Sports Health. 2017;9(5):436-443. doi:10.1177/1941738117704153
- Peitz M, Behringer M, Granacher U. A systematic review on the effects of resistance and plyometric training on physical fitness in youth- What do comparative studies tell us? PLoS One. 2018 Oct 10;13(10):e0205525. doi: 10.1371/journal.pone.0205525. Erratum in: PLoS One. 2018 Nov 14;13(11):e0207641. PMID: 30304033; PMCID: PMC6179270.
- Webster KE, Hewett TE. Meta-analysis of meta-analyses of anterior cruciate ligament injury reduction training programs. J Orthop Res. 2018 Oct;36(10):2696-2708. doi: 10.1002/jor.24043. Epub 2018 Jun 13. PMID: 29737024.
- Mason-Mackay AR, Whatman C, Reid D. The effect of reduced ankle dorsiflexion on lower extremity mechanics during landing: A systematic review. J Sci Med Sport. 2017 May;20(5):451-458. doi: 10.1016/j.jsams.2015.06.006. Epub 2015 Jun 15. PMID: 26117159.
- Gabbett TJ. The training-injury prevention paradox: should athletes be training smarter and harder?. Br J Sports Med. 2016;50(5):273-280. doi:10.1136/bjsports-2015-095788
- Gabbett TJ, Nassis GP, Oetter E, Pretorius J, Johnston N, Medina D, Rodas G, Myslinski T, Howells D, Beard A, Ryan A. The athlete monitoring cycle: a practical guide to interpreting and applying training monitoring data. Br J Sports Med. 2017 Oct;51(20):1451-1452. doi: 10.1136/bjsports-2016-097298. Epub 2017 Jun 23. PMID: 28646100.
- Debien PB, Timoteo TF, Gabbett TJ, Bara Filho MG. Training-Load Management in Rhythmic Gymnastics: Practices and Perceptions of Coaches, Medical Staff, and Gymnasts. Int J Sports Physiol Perform. 2022 Jan 11:1-11. doi: 10.1123/ijspp.2021-0279. Epub ahead of print. PMID: 35016155.
- Thomas E, Bianco A, Paoli A, Palma A. The Relation Between Stretching Typology and Stretching Duration: The Effects on Range of Motion. Int J Sports Med. 2018 Apr;39(4):243-254. doi: 10.1055/s-0044-101146. Epub 2018 Mar 5. PMID: 29506306.
- O’SullivanK, McAuliffe S, DeBurca N. The effects of eccentric training on lower limb flexibility: a systematic review. British Journal of Sports Medicine 2012;46:838-845.
- Weppler CH, Magnusson SP. Increasing muscle extensibility: a matter of increasing length or modifying sensation? Phys Ther. 2010 Mar;90(3):438-49. doi: 10.2522/ptj.20090012. Epub 2010 Jan 14. PMID: 20075147.
- Noyes F.R. Noyes Knee Disorders: Surgery, Rehabilitation, Clinical Outcomes. 2010. Elsivier. Philadelphia, USA.
- Flandry F, Hommel G. Normal anatomy and biomechanics of the knee. Sports Med Arthrosc Rev. 2011 Jun;19(2):82-92. doi: 10.1097/JSA.0b013e318210c0aa. PMID: 21540705.
- Wilk KE, Macrina LC, Reinold MM. Rehabilitation following Microfracture of the Knee. Cartilage. 2010 Apr;1(2):96-107. doi: 10.1177/1947603510366029. PMID: 26069540; PMCID: PMC4297050.
- Wilk KE, Macrina LC, Cain EL, Dugas JR, Andrews JR. Recent advances in the rehabilitation of anterior cruciate ligament injuries. J Orthop Sports Phys Ther. 2012 Mar;42(3):153-71. doi: 10.2519/jospt.2012.3741. Epub 2012 Feb 29. PMID: 22382825.
- Wilk KE, Davies GJ, Mangine RE, Malone TR. Patellofemoral disorders: a classification system and clinical guidelines for nonoperative rehabilitation. J Orthop Sports Phys Ther. 1998 Nov;28(5):307-22. doi: 10.2519/jospt.1998.28.5.307. PMID: 9809279.
- Dye SF. The pathophysiology of patellofemoral pain: a tissue homeostasis perspective. Clin Orthop Relat Res. 2005 Jul;(436):100-10. doi: 10.1097/01.blo.0000172303.74414.7d. PMID: 15995427.
- Laidlaw MS, Diduch DR. Current Concepts in the Management of Patellar Instability. Indian J Orthop. 2017 Sep-Oct;51(5):493-504. doi: 10.4103/ortho.IJOrtho_164_17. PMID: 28966372; PMCID: PMC5609370.
- Laidlaw MS, Diduch DR. Current Concepts in the Management of Patellar Instability. Indian J Orthop. 2017;51(5):493-504. doi:10.4103/ortho.IJOrtho_164_17
- Mace J, Bhatti W, Anand S. Infrapatellar fat pad syndrome: a review of anatomy, function, treatment and dynamics. Acta Orthop Belg. 2016 Mar;82(1):94-101. PMID: 26984660.
- Borja MJ, Jose J, Vecchione D, Clifford PD, Lesniak BP. Prefemoral fat pad impingement syndrome: identification and diagnosis. Am J Orthop (Belle Mead NJ). 2013 Jan;42(1):E9-11. PMID: 23431544.
- Geisler PR. Iliotibial Band Pathology: Synthesizing the Available Evidence for Clinical Progress. J Athl Train. 2020 Dec 22. doi: 10.4085/JAT0548-19. Epub ahead of print. PMID: 33351908.
- Strauss EJ, Kim S, Calcei JG, Park D. Iliotibial band syndrome: evaluation and management. J Am Acad Orthop Surg. 2011 Dec;19(12):728-36. doi: 10.5435/00124635-201112000-00003. PMID: 22134205.
- Chaudhry H, Schleip R, Ji Z, Bukiet B, Maney M, Findley T. Three-dimensional mathematical model for deformation of human fasciae in manual therapy. J Am Osteopath Assoc. 2008 Aug;108(8):379-90. doi: 10.7556/jaoa.2008.108.8.379. PMID: 18723456.
- McKay J, Maffulli N, Aicale R, Taunton J. Iliotibial band syndrome rehabilitation in female runners: a pilot randomized study. J Orthop Surg Res. 2020;15(1):188. Published 2020 May 24. doi:10.1186/s13018-020-01713-7
- Arnold A, Thigpen CA, Beattie PF, Kissenberth MJ, Shanley E. Overuse Physeal Injuries in Youth Athletes: Risk Factors, Prevention, and Treatment Strategies. Sports Health. 2017;9(2):139-147. doi:10.1177/1941738117690847
- Caine D, DiFiori J, Maffulli N. Physeal injuries in children’s and youth sports: reasons for concern?. Br J Sports Med. 2006;40(9):749-760. doi:10.1136/bjsm.2005.017822
- Wilk KE, Arrigo CA. Rehabilitation Principles of the Anterior Cruciate Ligament Reconstructed Knee: Twelve Steps for Successful Progression and Return to Play. Clin Sports Med. 2017 Jan;36(1):189-232. doi: 10.1016/j.csm.2016.08.012. PMID: 27871658.
- Wilk KE. Anterior Cruciate Ligament Injury Prevention and Rehabilitation: Let’s Get It Right. J Orthop Sports Phys Ther. 2015 Oct;45(10):729-30. doi: 10.2519/jospt.2015.0109. PMID: 26424574.
- ArdernCL, Ekås GR, Grindem H, et al2018 International Olympic Committee consensus statement on prevention, diagnosis and management of paediatric anterior cruciate ligament (ACL) injuries. British Journal of Sports Medicine 2018;52:422-438.
- Andrews K, Lu A, Mckean L, Ebraheim N. Review: Medial collateral ligament injuries. J Orthop. 2017 Aug 15;14(4):550-554. doi: 10.1016/j.jor.2017.07.017. PMID: 28878515; PMCID: PMC5581380.
- Naqvi U, Sherman AL. Medial Collateral Ligament Knee Injuries. 2022 Jan 2. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 28613747.
- Encinas-Ullán CA, Rodríguez-Merchán EC. Isolated medial collateral ligament tears: An update on management. EFORT Open Rev. 2018 Jul 2;3(7):398-407. doi: 10.1302/2058-5241.3.170035. PMID: 30233815; PMCID: PMC6129956.
- Raj MA, Mabrouk A, Varacallo M. Posterior Cruciate Ligament Knee Injuries. 2021 Aug 14. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 28613477.
- Pache S, Aman ZS, Kennedy M, et al. Posterior Cruciate Ligament: Current Concepts Review. Arch Bone Jt Surg. 2018;6(1):8-18.
- Kramer DE, Miller PE, Berrahou IK, Yen YM, Heyworth BE. Collateral Ligament Knee Injuries in Pediatric and Adolescent Athletes. J Pediatr Orthop. 2020 Feb;40(2):71-77. doi: 10.1097/BPO.0000000000001112. PMID: 31923166.
- Smoak JB, Matthews JR, Vinod AV, Kluczynski MA, Bisson LJ. An Up-to-Date Review of the Meniscus Literature: A Systematic Summary of Systematic Reviews and Meta-analyses. Orthop J Sports Med. 2020 Sep 9;8(9):2325967120950306. doi: 10.1177/2325967120950306. PMID: 32953923; PMCID: PMC7485005.
- Logerstedt DS, Scalzitti DA, Bennell KL, Hinman RS, Silvers-Granelli H, Ebert J, Hambly K, Carey JL, Snyder-Mackler L, Axe MJ, McDonough CM. Knee Pain and Mobility Impairments: Meniscal and Articular Cartilage Lesions Revision 2018. J Orthop Sports Phys Ther. 2018 Feb;48(2):A1-A50. doi: 10.2519/jospt.2018.0301. PMID: 29385940.
- Li J, Zhu W, Gao X, Li X. Comparison of Arthroscopic Partial Meniscectomy to Physical Therapy following Degenerative Meniscus Tears: A Systematic Review and Meta-analysis. Biomed Res Int. 2020 Mar 3;2020:1709415. doi: 10.1155/2020/1709415. PMID: 32190650; PMCID: PMC7073498.
- CookJL, Purdam CR. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. British Journal of Sports Medicine 2009;43:409-416.
- Rees JD, Maffulli N, Cook J. Management of Tendinopathy. The American Journal of Sports Medicine. 2009;37(9):1855-1867. doi:10.1177/0363546508324283
- Cardoso TB, Pizzari T, Kinsella R, Hope D, Cook JL. Current trends in tendinopathy management. Best Pract Res Clin Rheumatol. 2019 Feb;33(1):122-140. doi: 10.1016/j.berh.2019.02.001. Epub 2019 Mar 8. PMID: 31431267.
- Malliaras P, Cook J, Purdam C, Rio E. Patellar Tendinopathy: Clinical Diagnosis, Load Management, and Advice for Challenging Case Presentations. J Orthop Sports Phys Ther. 2015 Nov;45(11):887-98. doi: 10.2519/jospt.2015.5987. Epub 2015 Sep 21. PMID: 26390269.
- Reinking MF. CURRENT CONCEPTS IN THE TREATMENT OF PATELLAR TENDINOPATHY. Int J Sports Phys Ther. 2016;11(6):854-866.
- Figueroa D, Figueroa F, Calvo R. Patellar Tendinopathy: Diagnosis and Treatment. J Am Acad Orthop Surg. 2016 Dec;24(12):e184-e192. doi: 10.5435/JAAOS-D-15-00703. PMID: 27855131.
- Sederberg M, LaMarche L, Skinner L, Cushman DM. Distal semimembranosus tendinopathy: A narrative review. PM R. 2021 Jul 4. doi: 10.1002/pmrj.12667. Epub ahead of print. PMID: 34218525.
- Heiderscheit BC, Sherry MA, Silder A, Chumanov ES, Thelen DG. Hamstring strain injuries: recommendations for diagnosis, rehabilitation, and injury prevention. J Orthop Sports Phys Ther. 2010 Feb;40(2):67-81. doi: 10.2519/jospt.2010.3047. PMID: 20118524; PMCID: PMC2867336.
- Reinold MM, Wilk KE, Macrina LC, Dugas JR, Cain EL. Current concepts in the rehabilitation following articular cartilage repair procedures in the knee. J Orthop Sports Phys Ther. 2006 Oct;36(10):774-94. doi: 10.2519/jospt.2006.2228. PMID: 17063839.
- Wilk KE, Macrina LC, Reinold MM. Rehabilitation following Microfracture of the Knee. Cartilage. 2010 Apr;1(2):96-107. doi: 10.1177/1947603510366029. PMID: 26069540; PMCID: PMC4297050.
- Camp CL, Stuart MJ, Krych AJ. Current concepts of articular cartilage restoration techniques in the knee. Sports Health. 2014 May;6(3):265-73. doi: 10.1177/1941738113508917. Erratum in: Sports Health. 2014 Nov;6(6):NP1. Erratum in: Sports Health. 2014 Nov/Dec;6(6):NP1. PMID: 24790697; PMCID: PMC4000472.
- Palmieri-Smith RM, Kreinbrink J, Ashton-Miller JA, Wojtys EM. Quadriceps inhibition induced by an experimental knee joint effusion affects knee joint mechanics during a single-legged drop landing. Am J Sports Med. 2007 Aug;35(8):1269-75. doi: 10.1177/0363546506296417. Epub 2007 Jan 23. PMID: 17244901.
- Novaretti JV, Franciozi CE, Forgas A, Sasaki PH, Ingham SJM, Abdalla RJ. Quadriceps Strength Deficit at 6 Months After ACL Reconstruction Does Not Predict Return to Preinjury Sports Level. Sports Health. 2018 May/Jun;10(3):266-271. doi: 10.1177/1941738118759911. Epub 2018 Feb 27. PMID: 29485941; PMCID: PMC5958456.
- Powers CM, Ho KY, Chen YJ, Souza RB, Farrokhi S. Patellofemoral joint stress during weight-bearing and non-weight-bearing quadriceps exercises. J Orthop Sports Phys Ther. 2014 May;44(5):320-7. doi: 10.2519/jospt.2014.4936. Epub 2014 Mar 27. PMID: 24673446.
- Kaya D, Citaker S, Kerimoglu U, Atay OA, Nyland J, Callaghan M, Yakut Y, Yüksel I, Doral MN. Women with patellofemoral pain syndrome have quadriceps femoris volume and strength deficiency. Knee Surg Sports Traumatol Arthrosc. 2011 Feb;19(2):242-7. doi: 10.1007/s00167-010-1290-2. Epub 2010 Oct 15. PMID: 20953760.
- Crossley KM, Thancanamootoo K, Metcalf BR, Cook JL, Purdam CR, Warden SJ. Clinical features of patellar tendinopathy and their implications for rehabilitation. J Orthop Res. 2007 Sep;25(9):1164-75. doi: 10.1002/jor.20415. PMID: 17469196.
- Stensrud S, Risberg MA, Roos EM. Effect of exercise therapy compared with arthroscopic surgery on knee muscle strength and functional performance in middle-aged patients with degenerative meniscus tears: a 3-mo follow-up of a randomized controlled trial. Am J Phys Med Rehabil. 2015 Jun;94(6):460-73. doi: 10.1097/PHM.0000000000000209. PMID: 25299520.
- Beris AE, Lykissas MG, Kostas-Agnantis I, Manoudis GN. Treatment of full-thickness chondral defects of the knee with autologous chondrocyte implantation: a functional evaluation with long-term follow-up. Am J Sports Med. 2012 Mar;40(3):562-7. doi: 10.1177/0363546511428778. Epub 2011 Dec 2. PMID: 22138109
- Reinold MM, Wilk KE, Reed J, Crenshaw K, Andrews JR. Interval sport programs: guidelines for baseball, tennis, and golf. J Orthop Sports Phys Ther. 2002 Jun;32(6):293-8. doi: 10.2519/jospt.2002.32.6.293. PMID: 12061709
- Watson AM. Sleep and Athletic Performance. Curr Sports Med Rep. 2017 Nov/Dec;16(6):413-418. doi: 10.1249/JSR.0000000000000418. PMID: 29135639
- Beelen M, Burke LM, Gibala MJ, van Loon L JC. Nutritional strategies to promote postexercise recovery. Int J Sport Nutr Exerc Metab. 2010 Dec;20(6):515-32. doi: 10.1123/ijsnem.20.6.515. PMID: 21116024
- Sands WA, McNeal JR, Murray SR, Stone MH. Dynamic Compression Enhances Pressure-to-Pain Threshold in Elite Athlete Recovery: Exploratory Study. J Strength Cond Res. 2015 May;29(5):1263-72. doi: 10.1519/JSC.0000000000000412. PMID: 24531439




")


